ProAxsis ProteaseTag® Active Neutrophil Elastase Immunoassay
$0.00
Neutrophil elastase (NE) is a protein biomarker of infection and inflammation is shown to correlate with the severity of several respiratory diseases such as cystic fibrosis, COPD and bronchiectasis. This establishes NE as a frequently used COPD biomarker and CF biomarker for research. NE has long been used as an endpoint in clinical studies aimed at evaluating the efficacy of new anti-elastase inhibitors (neutrophil elastase inhibitors) or other anti-inflammatory therapies.
Applications
The molecular mechanisms that drive chronic lung disease are heterogenetic. To evolve past a “one drug fits all approach”, and towards a more individualized and precise approach, pharmaceutical companies are focusing on drugs that address each etiology within a disease. Hence, endotypes, which are the distinct pathobiological mechanisms driving disease, have come to the forefront in drug design. The endotype approach is also needed for assessing individuals for drug development.
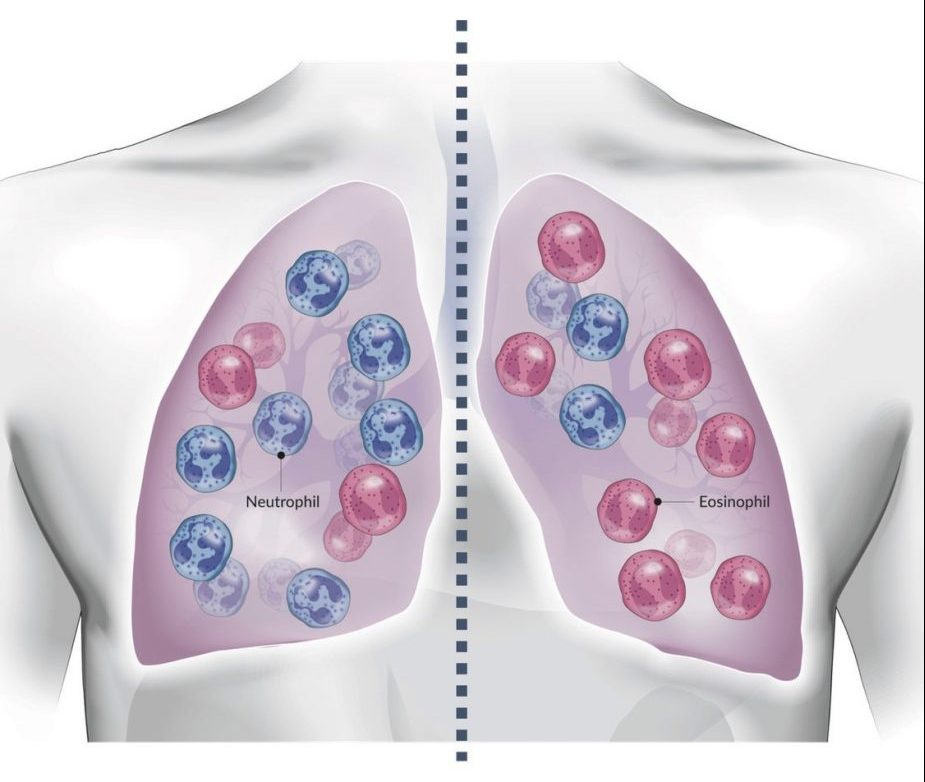
While many cell types can be accounted for in a diseased lung, there is usually one cell type that is the predominate driver of disease. This cell type can vary within a disease and can also change over the course of the disease. This makes endotyping an essential step to identify the distinct inflammatory cell type driving the disease in order to study the disease.
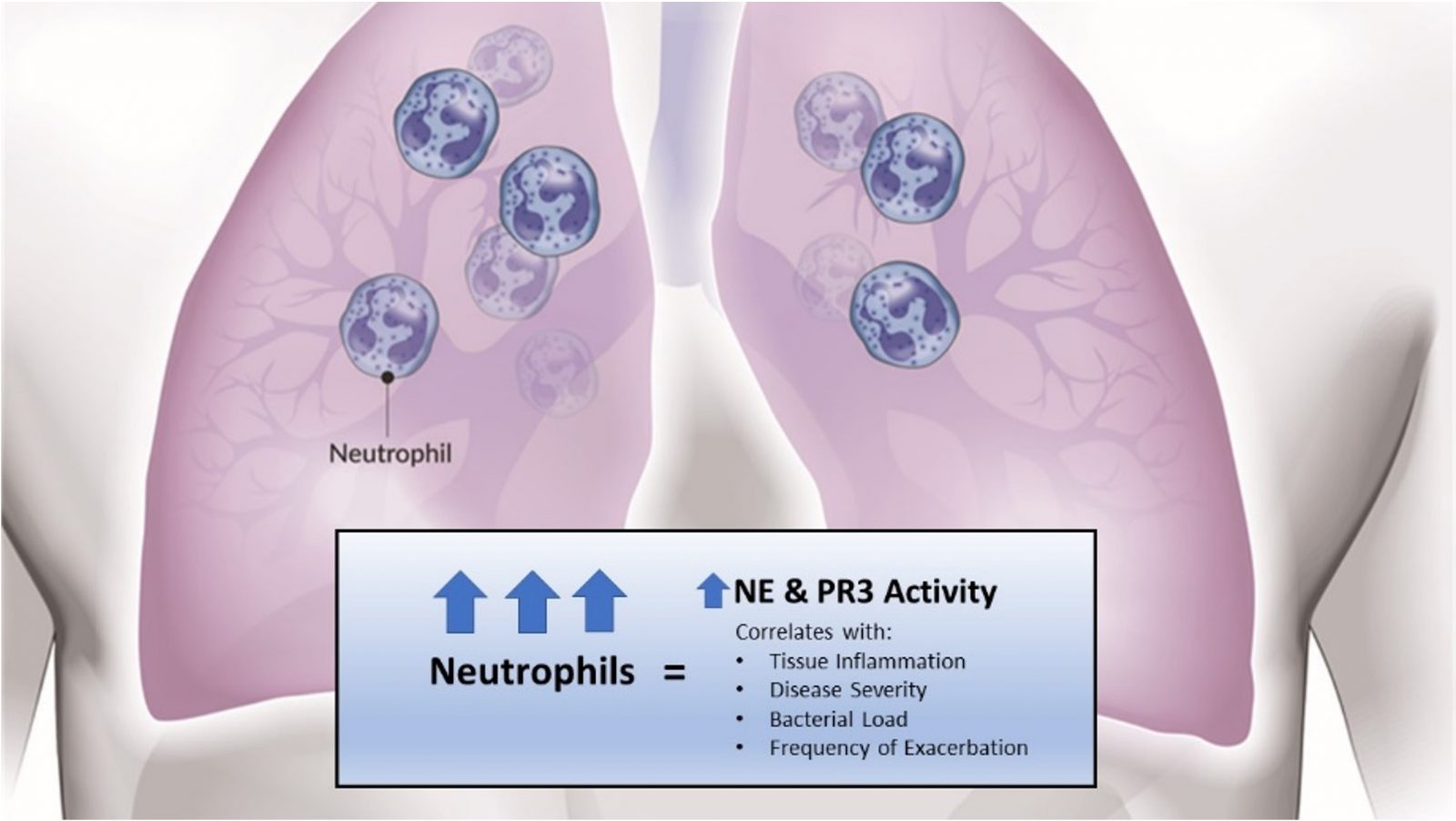
COPD, bronchiectasis, and asthma are most commonly characterized as eosinophilic or neutrophilic endotypes. Neutrophil elastase and proteinase 3 are proteases produced by neutrophils. When released, they facilitate a cycle of tissue damage and inflammation, driving pathology and disease. Measuring the activity levels of neutrophil elastase provides a specific and accurate assessment of neutrophil-driven disease to determine individual endotypes. This makes neutrophil elastase activity measurement an effective tool for drug development studies involving targets that inhibit neutrophil activity.
In addition to endotyping, neutrophil elastase measurement can function as a clinical trial endpoint for general inflammation in lung disease. Inflammation is a hallmark of chronic lung diseases and an important piece to understand when evaluating drug effectiveness. Decreasing lung-specific inflammation is a key strategy for pharmaceutical targets. Currently, the FEV1/FVC ratio is the primary endpoint during pulmonary drug development studies, but does not capture a complete picture of a disease state. Cytokine measurements are frequently recorded, but may not be specific to lung inflammation. Mechanistic markers of inflammation, like neutrophil elastase, can be detected earlier and indicate improvements in outcomes.
ProAxsis offers products that have proven to be valuable in enrolling, stratifying, and studying effectiveness of respiratory drugs in development. The ready-to-use kits offer a sensitive, reliable, and accurate read-out of neutrophil elastase and proteinase 3 activity in sputum or bronchoalveolar lavage (BAL). Neutrophil elastase and proteinase 3 activity levels correlate with disease severity, time to next exacerbation, and bacterial load. From an endotyping perspective, they are also global mechanistic markers of neutrophil-driven inflammatory states.
Read more about NE as a neutrophil serine proteases (NSP) and biomarker.
Principle of the Assay
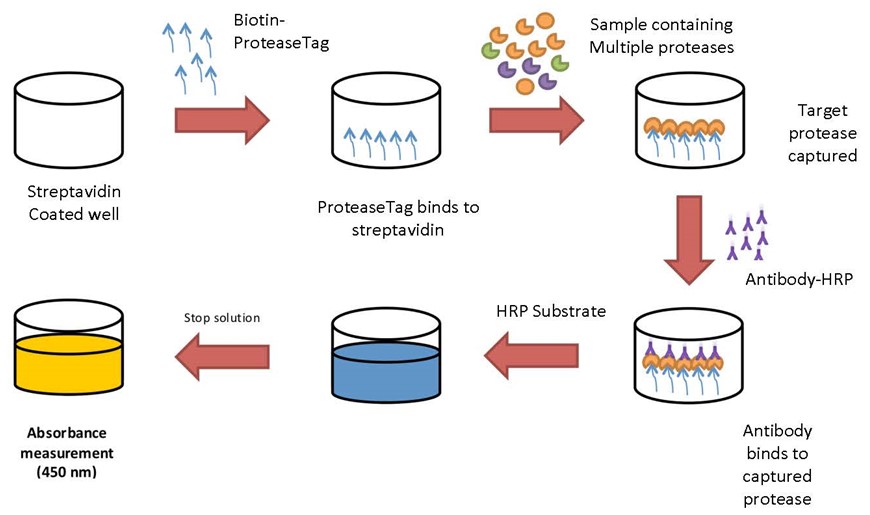
The ProteaseTag® Active NE Immunoassay utilizes ProteaseTag® technology to specifically detect and quantify active NE. The activity assay is a more specific alternative to a standard antigen or a total neutrophil elastase assay.
During a short incubation, the NE-Tag is coated onto the immunoassay plate before washing to remove excess. Standards and samples are added, and the NE-Tag will interact with the active site of NE during a second incubation step. Active NE present in the solutions will irreversibly bind to the NE-Tag while latent and inhibitor bound NE will be removed by washing. A horseradish peroxidase (HRP) conjugated anti-NE antibody is added to each test well and incubated. This detection antibody attaches to bound NE with unbound antibody subsequently removed by washing. A color forming substrate containing TMB is added to each test well and reacts with HRP to generate a blue colored product. This enzymatic reaction is subsequently stopped by the addition of acidic stop solution to each test well (a yellow solution is formed). The color intensity (absorbance) is read at 450 nm using a plate reader.
Sufficient reagents are provided to allow for two standard curves
Freezer Box Components (stored at -20°C)
| NE-Tag | 1 vial containing 4 μl (concentration 10 mM) of capture probe in DMF |
|---|---|
| NE Standard | 2 vials containing 6 μl of NE (concentration 100 μg/ml) in an acidic buffer. *Each vial can only be used once |
| NE Conjugate | 1 vial containing 25 μl of anti-human neutrophil elastase antibody conjugated to HRP in a stability solution |
Main Box Components (stored at 2-8°C)
| Immunoassay Plate | 96 well strep coated microtiter plate (pre-blocked) |
|---|---|
| NE Wash Buffer A Concentrate | 24 ml of a 25-fold concentration of buffered surfactant with preservatives |
| NE Wash Buffer B Concentrate | 8 ml of a 25-fold concentration of buffer with preservatives |
| NE Standard Diluent | 15 ml of buffer with preservatives (ready to use) |
| NE Reagent Diluent | 2 x 13 ml of buffered surfactant with preservatives (ready to use) |
| TMB Substrate | 12 mL of tetramethylbenzidine solution |
| Stop Solution | 6 mL of 2N sulfuric acid |
| Plate Sealers | 4 adhesive strips |
| Format | 96 well |
|---|---|
| Species | Human |
| Sample | Sputum, bronchial alveolar lavage fluid (BALF), wound exudate |
| Range | 15.625 – 1000 ng/ml |
| LOD | 7.2 ng/ml |
| Specificity | Only detects active NE |
| Run Time | 130 min of incubation |
| Cross Reactivity | Reactive with other species, but no official testing results provided |
| Standard Source | Native protein |