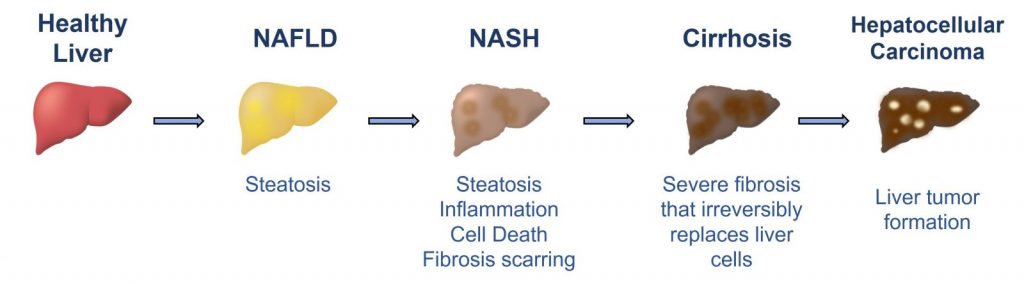
Non-alcoholic fatty liver disease (NAFLD) is caused by a buildup of fat in the liver (steatosis). NAFLD is the most common chronic liver disease in western populations, affecting 25% of the adult population in the United States. NAFLD can lead to liver inflammation (steatohepatitis) and damaging liver scarring (fibrosis). The more severe form of NAFLD is termed Non-alcoholic steatohepatitis (NASH). NASH is defined by chronic liver inflammation, hepatocyte death, and variable degrees of fibrosis. NASH can progress to stages of advanced fibrosis, cirrhosis, hepatocellular carcinoma, and ultimately, liver failure. NASH is rapidly becoming the leading cause of liver transplantation in the United States and is prevalent in about 5% of adults in the United States.
There are few outward symptoms of NAFLD and NASH. As liver disease progresses, symptoms may include fatigue, pain in the upper right abdomen, rapid bleeding and/or bruising, nausea, loss of appetite, swelling, jaundice, and confusion. Risk factors associated with NASH include obesity, type 2 diabetes, and metabolic syndrome.
Diagnosis
NAFLD and NASH diagnosis begins with a physical exam and routine blood tests for liver enzymes, such as alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Imaging via MRI or ultrasound technologies may be used to measure fat accumulation and liver fibrosis. The gold standard for NASH diagnosis is through liver biopsy analysis. Histological characteristics of NASH include macrovesicular steatosis, hepatocyte ballooning, lobular inflammation, apoptotic bodies, and Mallory-Denk bodies. Fibrosis can vary and is not required for NASH diagnosis.
Scoring systems have been developed to aid in the histological evaluation of liver biopsies. The commonly used NASH CRN scoring system is comprised of the NAFLD activity score (NAS) and fibrosis stage:
- The NAFLD Activity Score (NAS) correlates with NASH disease activity and is calculated based on the histological appearance of hepatocyte ballooning, steatosis, and inflammation. The NAS is computed on a scale of 0-8, with scores >5 indicating definite steatohepatitis.
- The fibrosis stage reflects liver disease progression on a scale of F0-F4 and is associated with prognosis. F0 correlates with no fibrosis detected in the biopsy sample and a score of F4 designates cirrhosis, which is a late stage of scarring that impairs liver function.
During clinical trials for NASH-targeted therapeutics, the NAS and the fibrosis stage are used to measure changes in NASH and fibrosis as a means to support clinical trial endpoints. The concept is that the NAS and the stage of fibrosis, when analyzed collectively, indicate the speed that the disease is progressing, together with the extent of liver damage within the biopsy sample. The histological effect, when calculated by the NAS and the fibrosis stage over the time course of a clinical trial, reveals the ability or inability of a NASH drug to meet clinical trial endpoints. While the histological scoring systems are suitable as semi-quantitative ways of analyzing biopsies, they were not designed to be effective tools for evaluating responsiveness to therapeutic interventions and have left a frustrating gap for the approval of potential NASH drugs.
There are several challenges regarding the use of liver biopsies in NASH clinical trials: Liver biopsies carry high intra- and inter-observer variability. This may drive inconsistent pathology interpretations of liver biopsies. Furthermore, NASH pathogenesis within the liver is not homogeneous, making the diagnostic potential of a single biopsy complex, difficult, and even incomplete. Added to that are the considerable cost and non-negligible risk of medical complications associated with liver biopsies.
Non-Invasive Testing
Although not yet widely available for clinical diagnostic use, there is a great need for testing options for NASH that minimize risk and are less invasive than liver biopsy analysis. Non-invasive tests (NITs) are tools for determining and monitoring NASH and fibrosis stage using methods that are repeatable, non-invasive, accessible, and cost less than liver biopsies. Due to their simplicity and repeatability, NITs can be used to monitor the effects of NASH drug treatments including the regression or reversal of fibrosis and steatosis over time, even in shorter duration trials when repeat liver biopsies are not feasible or when histology may not adequately reflect the effect of a drug candidate. However, the impact and consistency of non-invasive testing and retesting are incompletely documented and require further research.
Table 1 outlines NITs and algorithms that measure NASH activity and/or stage of liver fibrosis. Data inputs are either blood-based, imaging-based, or both. Each NIT and algorithm contains unique components that range in complexity, cost, and accessibility.
| Non-Invasive Tests and Algorithms | Components / Technology | Method | Utility | NASH | Fibrosis |
| Cytokeratin-18 (CK18) | cytokeratin-18 (CK18) M65® and M30® | Blood-Based | Serum CK18 (M65®) measures total hepatocyte death and cCK18 (M30®) measures hepatocyte apoptosis. | ✓ | |
| Enhanced Liver Fibrosis (ELF)™ | hyaluronic acid (HA), PIIINP, TIMP-1 | Blood-Based | ELF™ correlates with fibrosis stage during chronic liver disease. | ✓ | |
| Fibrosis-4 (FIB-4) | age, AST, ALT, platelet count | Blood-Based | FIB-4 estimates fibrosis stage. | ✓ | |
| FICK-3 / FIC-22 | FIB-4, cCK18, HOMA | Blood-Based | Fick-3 / FIC-22 is a predictor of NASH and liver fibrosis. | ✓ | ✓ |
| LiverFast™ | α2M, ApoA1, total bilirubin, GGT, ALT, AST, fasting glucose, triglyceride, total cholesterol | Blood-Based | LiverFast™ determines liver fibrosis, disease activity, and steatosis stage. | ✓ | ✓ |
| MACK-3 | HOMA (fasting glucose and fasting insulin), AST, CK18 | Blood-Based | MACK-3 is an indicator of NASH activity and fibrosis. | ✓ | ✓ |
| Metabolomics Advanced StEatohepatits Fibrosis Score (MASEF) | 12 lipids, BMI, AST, ALT | Blood-Based | The MASEF score identifies high-risk NASH and significant liver fibrosis. | ✓ | ✓ |
| NAFLD Fibrosis Score (NFS) | age, BMI, IFG, AST/ALT ratio, platelet count, and albumin | Blood-Based | NFS provides an estimate of liver fibrosis. | ✓ | |
| NIS4® | miR34a, alpha-2-macroglobulin, HbA1c, YKL-40/Chitinase-3-like protein 1 | Blood-Based | The NIS4® identifies NASH, NAS ≥ 4, F≥2. | ✓ | ✓ |
| OWLiver® test | Rapid throughput of small molecule metabolites | Blood-Based | The OWLiver® test can distinguish between NAFLD and NASH. | ✓ | |
| Pro-peptide of type III collagen (Pro-C3) | pro-peptide of type III collagen (Pro-C3) | Blood-Based | PRO-C3 correlates with fibrosis. | ✓ | |
| Z-Score | AST, HbA1C, CK18 | Blood-Based | The composite Z-score algorithm correlates with histological improvement in NASH. | ✓ | ✓ |
| Corrected T1 (cT1) | MRI | Imaging | cT1 correlates with ballooning, fibrosis, and NAS. | ✓ | ✓ |
| Fibroscan® | ultrasound transient elastography | Imaging | Fibroscan® measures fibrosis and steatosis. | ✓ | |
| Magnetic Resonance Elastography (MRE) | MRI and ultrasound | Imaging | MRE detects stiffening of the liver caused by fibrosis and inflammation. | ✓ | |
| Magnetic resonance imaging derived proton density fat fraction (MRI-PDFF) | MRI | Imaging | MRI-PDFF measures liver fat content and detects individuals with NASH, NAS ≥ 4 and F ≥ 2. | ✓ | |
| Shear wave elastography (SWE) | ultrasound elastography | Imaging | SWE measures organ stiffness. | ✓ | |
| Fibroscan®-AST (FAST) | VCTE/LSM (fibrosis), CAP (steatosis), AST (activity) | Imaging + Blood-based | FAST predicts active NASH with fibrosis. | ✓ | ✓ |
| MRI and AST (MAST) | MRI and AST | Imaging + Blood-based | MAST detects individuals with NASH, NAS ≥ 4 and F ≥ 2. | ✓ | ✓ |
Table 1: Non-invasive tests and algorithms that are being used to investigate NASH and liver fibrosis stage. Blood-based algorithms are shaded in blue, imaging-based tests are shaded in orange, and combinations of imaging and blood-based tests are shaded in green.
There are two common categories of NAFLD/NASH biomarkers, diagnostic biomarkers and treatment response biomarkers. Many NITs offer dual utility as both diagnostic biomarkers and treatment response biomarkers.
Diagnostic biomarkers provide a snapshot of the liver disease state. Diagnostic biomarkers can also be used to screen enrollment populations during clinical trials. Preliminary screening is beneficial to clinical trials to avoid unnecessary biopsies and enrich populations for individuals that meet enrollment criteria. Diagnostic biomarker tests include MACK-3, ELF™, FIB-4, Fibroscan®, and NIS4®. For disease prognosis, ELF™ was the first test to receive FDA approval for predicting progression to cirrhosis and liver-related events in NASH patients with advanced fibrosis.
Treatment response biomarkers require measurements over time and indicate the progression or regression of the liver disease. This type of non-invasive analysis is particularly valuable during NASH clinical trials where disease regression over time frequently falls below the level of detection that can accurately be measured by liver biopsy. Treatment response biomarkers include CK18 (M30® and M65®), Z-Score, NIS4®, Pro-C3, Fibroscan®, FAST, and ALT.
While the exploration of novel NASH biomarkers is valuable and needed, the field remains in infancy and contains obstacles to overcome during NASH drug development and clinical use. The mechanisms underlying NASH are multifactorial, and hence so are the approaches taken during pharmaceutical development. Each pharmaceutical company invested in NASH drug development has conducted independent clinical trials and has accumulated unique biomarker data to evaluate their disease mechanisms of interest. This independent approach has resulted in a scattering of data across the NASH landscape with no clear “best in practice” approach for diagnostic or treatment response biomarkers.
To address this, several consortia have formed to evaluate and prioritize the best biomarkers to adopt into the NASH drug development space and for clinical practice. Two multicenter consortia have been created, one in Europe and the other in the United States (US), to systematically compare the performance of NITs against the liver biopsy gold standard. LITMUS (Liver Investigation: Testing Marker Utility in Steatohepatitis) is supported by European efforts and NIMBLE (Non-Invasive Biomarkers of Metabolic Liver Disease) is a US-initiated study. An additional privately funded consortium named NAIL-NIT (NASH Consortium for the Assessment of Non-Invasive Testing in Monitoring Interventions and Treatment Response and Major Liver Related Outcomes) has recently been established to investigate associations between NITs and liver-related outcomes using NIT data accumulated during drug trials. Preliminary efforts are promising, but there are concerns surrounding inconsistencies and lack of coordination between the various consortia.
Therapeutics
Current NAFLD and NASH therapies
There are currently no FDA-approved treatments for NASH, driving an urgent need for the development of novel therapeutics and accelerated NASH clinical trials.
The Future of NAFLD and NASH Therapies
Clinical trials and randomized control trials are underway to investigate the efficacy of therapeutics to treat NAFLD and NASH. Key objectives of NAFLD and NASH therapies under investigation include targeting apoptosis, hepatic fat accumulation, inflammation, oxidative stress, microbiomes, and liver fibrosis.
Due to the requirement of paired liver biopsies for FDA approval of new NASH drugs, there is a significant and unfortunate bottleneck that is slowing the clinical trial process and entrance of NASH drugs into the market.
Biomarkers and Research
Non-invasive biomarkers are powerful research tools that probe the mechanisms underlying NAFLD and NASH. Imaging and blood-based biomarkers can be used to predict changes in liver histology as well as indicate early responses to treatment. Non-invasive biomarkers have potential to function as surrogates for histologic improvement in the liver, which could greatly aid in the achievement of histologic endpoints in NASH clinical trials. Many biomarkers are under investigation for use in NAFLD and NASH research and NASH clinical trials.
Click here for a full list of NAFLD and NASH biomarkers available from DiaPharma for use in NASH clinical trials. Continue reading below for a brief highlight and description of each NAFLD and NASH biomarker that we offer.
Cell death biomarkers
Cytokeratin-18 (CK18) is an intermediate filament protein that is expressed in epithelial cells, including hepatocytes. Aberrant hepatocyte apoptosis is a key feature and driver of NASH. Following hepatic injury, CK18 is released into the blood in a mechanism that is specific to cell death. M30® ELISA kits from VLV Bio measure an apoptosis-specific fragment, while the M65® ELISA kits measure total CK18. Elevated CK18 levels correlate with disease activity (NAS) and NASH progression. While CK18 is not a fibrosis marker per se, hepatocyte apoptosis plays an important role in the development of liver fibrosis, and CK18 levels have been shown to relate strongly with fibrosis stage and worsening of fibrosis.
Biomarkers that reflect liver histology
Multivariable modeling has demonstrated the ability of non-invasive biomarkers to specifically predict changes in liver histology during NASH pathogenesis and treatment. A composite Z-score has been developed that analyzes changes in AST, CK18, and hemoglobin A1C (HbA1c) levels to predict liver histologic responses. The biomarkers in the composite Z-score panel are accessible, inexpensive, and can be performed retrospectively on banked blood samples, giving them an advantage over liver biopsies.
Inflammation and Fibrosis biomarkers
C-Reactive Protein (CRP) is secreted from the liver and functions to activate the complement system after binding cell surface receptors on dead cells. CRP is elevated following inflammation, injury, or necrosis. CRP levels are elevated in individuals with NAFLD and NASH.
Fatty Acid Binding Protein (FABP) and Liver-type FABP (L-FABP) L-FABP is expressed in liver hepatocytes and leaks out of the cell following necrosis. Serum levels of L-FABP are increased in NASH and correlate with fibrosis and inflammation. FABP4 is expressed in adipocytes and FABP4 levels are elevated in NAFLD, insulin resistance, and type 2 diabetes.
Galectin-3 is in the lectin protein family and functions during cell growth, chemoattraction, cell cycle, and apoptosis. Expression of Galectin-3 is associated with chronic inflammation and fibrosis in NASH and cirrhosis.
Growth differentiation factor-15 (GDF-15) is a stress-induced cytokine. Transcript studies identified that GDF-15 expression is associated with fibrosis severity in NAFLD. Plasma GDF-15 concentrations are predictive of liver fibrosis and may have a role in the association between liver fibrosis in NAFLD and type 2 diabetes mellitus (T2DM).
Hyaluronic Acid (HA) is a component of the extracellular matrix throughout the body. Elevated HA levels correlate with the histological stage of fibrosis in the liver. Elevated HA levels indicate NASH with the presence of fibrosis and correlate with the fibrosis stage. In subjects with NASH but without fibrosis, HA levels can vary.
Lipocalin-2 (LCN2) / Neutrophil Gelatinase-associated Lipocalin (NGAL) is a glycoprotein that is released during states of inflammation. LCN2 levels are elevated in NASH in a role that promotes inflammation.
Mac-2 binding protein (Mac-2bp) is a secreted protein that functions as a ligand for Galectin-3. Mac-2bp is useful as an indicator of NASH, and chronic liver disease progression, and is predictive of NAFLD severity and stage of fibrosis.
Neutrophil Elastase (NE) is a serine protease that is released from neutrophils during inflammatory events. NE may be an indicator of inflammation and disease severity in NAFLD and NASH subjects.
Osteopontin (OPN) is an extracellular matrix protein that functions as a mediator of inflammation and fibrosis. Elevated serum levels of OPN are predictive of inflammation in NAFLD subjects and correlate with the fibrosis stage in NASH.
Periostin is a secreted extracellular matrix and cell adhesion protein. Early studies suggest that periostin serum levels may be elevated in NAFLD subjects, suggesting a role for periostin in mediating liver steatosis, inflammation, and fibrosis.
Proteinase 3 (PR3) is a serine protease located in polymorphonuclear neutrophils. PR3 functions to kill intracellular pathogens and degrade extracellular matrix components at inflammatory sites. PR3 serum levels are elevated in individuals with hepatic steatosis and are associated with NAFLD, NASH, and liver fibrosis.
Soluble CD163 (sCD163) is cell surface protein that is a marker of activated monocytes and macrophages. sCD163 levels can therefore reflect macrophage and monocyte recruitment to sites of tissue damage, which contribute to the pathogenesis of NAFLD and NASH.
Thrombospondin-2 (TSP2) mediates cell-to-cell and cell-to-matrix interactions. Population-based transcriptomic analysis showed that TSP2 is upregulated in NASH and stage F3 and F4 fibrosis. TSP2 protein levels correlate with NAS activity scores.
WNT3A and the Wnt signaling pathway are activated during liver fibrosis. WNT3a is an interesting biomarker for the detection of chronic liver injury, such as NAFLD and NASH.
Biomarkers of Metabolic Disorders and Adipokines
NASH is associated with disorders that affect insulin resistance, such as type 2 diabetes and obesity. Insulin and Intact Proinsulin are important indicators of diabetes, metabolic syndrome, and insulin resistance and hence make compelling biomarkers of metabolic changes in NASH.
Adiponectin is a hormone that is secreted from adipose cells and possesses anti-diabetic and anti-inflammatory functions. Decreased plasma adiponectin levels are associated with NASH.
Leptin is produced by adipocytes and is important for regulating body fat mass and fibrosis. Leptin levels correlate with liver steatosis severity in NASH individuals.
Plasminogen activator inhibitor-1 (PAI-1) is active in thrombotic, fibrinolytic, inflammatory, and metabolic pathways. Elevated plasma PAI-1 levels are associated with cardiovascular disease. NASH and NAFLD are associated with an increased risk for cardiovascular events and elevated levels of PAI-1 have been described in NAFLD and NASH patients. This suggests that PAI-1 may be an important biomarker of cardiovascular risk in NASH patients.
Retinol Binding Protein 4 (RBP4) is a retinol transporter protein that is a biomarker for inflammation, obesity, and insulin resistance. Serum levels of RBP4 are elevated in type 2 diabetes and are associated with increased cardiovascular disease.
Signaling Pathway Biomarkers
Asporin blocks TGF-beta signaling. Low levels of Asporin are reported in NAFLD and NASH subjects. Aspirin may be valuable as a treatment response biomarker for Vitamin E therapy.
Fibroblast growth factors FGF-19 and FGF-21 are activated during liver injury in NAFLD and are emerging biomarkers for NASH research.
Noggin antagonizes BMP signaling. Noggin serum levels are low in NAFLD patients. Noggin may be useful as a treatment response biomarker for Vitamin E therapy.