Blood sugar levels naturally rise after eating and drinking, prompting the pancreas to release insulin from specialized islet cells known as beta cells. Insulin plays a crucial role in regulating glucose transport from the bloodstream into cells, where it is used for energy and metabolic functions.
Diabetes is a condition that occurs when the body cannot adequately produce or respond to insulin. When insulin is not properly processed, or if cells develop resistance to insulin signaling, blood glucose levels become elevated, leading to a state known as hyperglycemia. Hyperglycemia is both a symptom of diabetes and a contributing factor to its progression. Hyperglycemia exacerbates insulin resistance and damages the insulin-secreting beta cells, driving beta cell dysfunction and reduced insulin production. Chronic hyperglycemia can lead to further complications including vascular endothelial damage, increased risk of infection, and microvascular complications.
The two most common types of diabetes are type 1 diabetes (T1D) and type 2 diabetes (T2D). T1D is an autoimmune disease in which the immune system attacks pancreatic beta cells, while T2D is characterized by the body’s inability to respond effectively to insulin. Dysfunctional beta cells are central to the clinical progression of both T1D and T2D, ultimately leading to reduced insulin production and subsequent hyperglycemia.
Given the important role of beta cells in the pathophysiology of diabetes, understanding the molecular processes that drive insulin synthesis, processing, and secretion is essential for identifying and developing effective treatments for T1D and T2D.
Beta Cell Function
Pancreatic beta cells are responsible for producing and secreting insulin in order to manage glucose homeostasis. Impaired beta cell function disrupts insulin production, processing, and secretion resulting in dangerous elevations of blood glucose levels. Beta cell dysfunction leads to an inability to effectively manage blood glucose levels, leading to well-characterized clinical indicators of diabetes.
Beta cell dysfunction is a defining feature of diabetes. Although the underlying mechanisms differ between T1D and T2D, beta cell functionality is compromised in both, contributing to damage and clinical outcomes associated with the diseases. Changes to beta cell function often precede clinical thresholds of diabetes, indicating that biomarkers of beta cell health can serve as early indicators of diabetes disease.
In both T1D and T2D, there is an initial latent phase during which beta cell function is either attacked or altered prior to clinical diagnosis. This emphasizes the importance of biomarkers of beta cell functionality as valuable tools for the early detection and intervention of diabetes.
The Insulin Pathway
Insulin is expressed and secreted by pancreatic beta cells. The process beings with the transcription of insulin mRNA, which is translated into a precursor called preproinsulin. Preproinsulin consists of a signal peptide, two chains (chain A and chain B) which later bond together to form insulin, and a C-peptide molecule (Fig 1A). The signal peptide directs preproinsulin to the endoplasmic reticulum (ER) for further processing. Within the ER, the signal peptide is cleaved, resulting in the formation of intact proinsulin (Fig 1B). The intact form of proinsulin contains chain A, chain B, and the C-peptide.
Following post-translational modifications in the Golgi apparatus, proinsulin is packaged into secretory vesicles (Fig 1C). Enzymatic cleavage by PC1, PC2, and carboxypeptidase E produces partially cleaved proinsulin isoforms, ultimately leading to the release of C-peptide and the mature form of insulin (Fig 1C-D). Stimulating events, such as elevated blood glucose levels, trigger the release of mature insulin and C-peptide into the bloodstream, initiating signaling cascades necessary for glucose uptake (Fig 1E).
When beta cells experience stress, insulin processing enzymes become overwhelmed and deficient in their ability to process proinsulin effectively. This leads to the accumulation of proinsulin, which can reach levels detectable in the blood (Table 1). Measurements of intact proinsulin and proinsulin intermediates in the blood serve as indicators of insulin processing defects that occur in stressed beta cells during the course of diabetes.
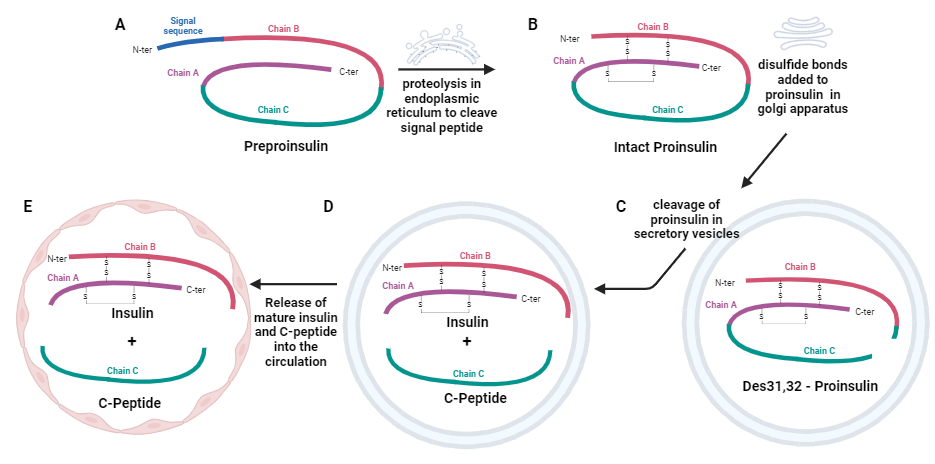
Fig 1. Insulin Pathway Components. Structure of preproinsulin (A), intact proinsulin (B), proinsulin isoforms (C), insulin and C-peptide (D), and final release of insulin and C-peptide into the bloodstream (E). Figure created with BioRender.com
Biomarkers of Beta Cell Function
Despite the similarities in appearance and nomenclature of these molecules, there are subtle yet important distinctions within the insulin pathway that must be considered when analyzing beta cell function, particularly in the context of diabetes research (Table 1).
- Preproinsulin serves as the earliest indicator of insulin processing. Although it is not commonly analyzed in clinical settings, measuring preproinsulin levels could provide insights into the dynamics of insulin processing in research studies.
- Proinsulin is used as a biomarker for assessing beta cell health, insulin processing, and insulin secretion capacity. It can be measured in two forms: intact proinsulin and total proinsulin.
- Intact proinsulin consists of chain A, chain B, and C-peptide molecules only. Cleaved proinsulin isoforms are excluded from this measurement.
- Total proinsulin includes intact proinsulin along with partially cleaved isoforms, such as Des31,32 proinsulin. Notably, Des31,32 proinsulin isoform has a longer half-life than intact proinsulin, which may lead to an overestimation of proinsulin levels.
- Insulin provides a direct readout on the insulin-secreting abilities of beta cells. Due to its rapid clearance from circulation by the liver, insulin has a short half-life.
- C-Peptide is cleaved from proinsulin and is considered functionally inert. It is frequently used as a marker of insulin secretion and beta cell functionality. It has a longer half-life than insulin, allowing for extended detection periods in the bloodstream.
A common approach to assessing beta functionality involves analyzing the ratios of components of the insulin pathway. Calculating these ratios provides insights into beta cell function that may be obscured when measuring individual pathway components in isolation.
- The insulin to C-peptide ratio (ICPR) reflects the amount of insulin secreted relative to C-peptide levels. Careful interpretation of the ICPR must be performed, as C-peptide has a slower metabolic clearance rate than insulin, potentially affecting the ratio’s accuracy.
- The proinsulin to C-peptide (PI:C) ratio and the proinsulin to insulin (PI/I) ratio can be calculated to evaluate the efficiency of proinsulin processing and secretion. When beta cells are dysfunctional, intact proinsulin levels accumulate in the blood while insulin and C-peptide levels decline. This results in a disproportionate ratio of intact proinsulin to C-peptide or insulin, indicating beta cell stress.
- Elevated PI/I ratios can indicate increased demand on beta cells for insulin secretion.
- Elevated PI:C can indicate beta cell dysfunction. Research studies focused on delaying the onset of clinical T1D have associated elevated PI:C with optimal therapeutic windows for teplizumab treatment.
| Term | Description | Healthy Physiological Location | Status during Beta Cell Dysfunction or Stress | Biomarker Indications |
| Preproinsulin | Precursor to proinsulin that contains a signal peptide | Beta cells | Impaired preproinsulin processing | Dynamics of insulin synthesis, processing, and secretion |
| Intact Proinsulin | Chain A, chain B, and C-peptide. Only complete Proinsulin molecules are measured. | Beta cells | Accumulation and elevation of proinsulin levels in the blood | Insulin processing, Insulin secretion, Beta cell stress and dysfunction |
| Total Proinsulin | Chain A, chain B, and C peptide. Total proinsulin measures intact proinsulin together with partially-cleaved proinsulin isoforms | Beta cells | Accumulation and elevation of proinsulin levels in the blood | The Des31,32 proinsulin isoform has a longer half-life than intact proinsulin which could give an overestimation of beta cell function. |
| Insulin | Activates signaling to enable the uptake of glucose into cells, Shorter half-life than C-Peptide | Secretory vesicles, Blood | Altered insulin processing, Reduced insulin secretion | Insulin processing, Insulin secretion, beta cell health |
| C-Peptide | Cleavage product of proinsulin, Longer half-life than insulin, Biologically inactive | Secretory vesicles, Blood | Altered insulin processing, Reduced C-peptide secretion | Insulin processing, Insulin secretion, beta cell health |
Beta Cell Dysfunction During Diabetes Disease
Type 1 Diabetes
T1D is an autoimmune disease that develops progressively over several stages, characterized by varying levels of immune activity and beta cell dysfunction.
- Stage 1 T1D: Autoimmunity with normal blood glucose: Identified by the presence of 2 or more autoantibodies
- Stage 2 T1D: Autoimmunity with abnormal blood glucose: Identified by the presence of 2 or more autoantibodies + dysglycemia
- Stage 3 T1D: Clinical T1D: Identified by the presence of 2 or more autoantibodies + hyperglycemia + clinical symptoms (excessive thirst, weight loss, fatigue, and more)
T1D features a long latent phase during which autoantibodies are present without clinical symptoms. As the immune system destroys beta cells in T1D, elevated levels of proinsulin can often be detected in the blood. This indicates early beta cell dysfunction, which is a hallmark of autoimmunity in T1D.
Individuals diagnosed with hyperglycemia may receive insulin treatment, which can sometimes lead to a temporary remission known as the honeymoon period. During this phase, beta cells may resume insulin production, possibly due to the rest provided by insulin therapy. However, not all patients experience this recovery, as some beta cells may be too damaged to regain functionality.
While insulin is an effective treatment for managing T1D, it does not address the underlying cause of the disease. Immunotherapies targeting the autoimmune attack on beta cells are under development. Teplizumab became the first drug approved in the U.S. to delay the onset of clinical T1D, receiving FDA approval in 2022 for the treatment of individuals with stage 2 T1D as young as 8 years old. Retrospective analysis of clinical study data has indicated that the PI:C ratio at the time of diagnosis correlates with response to Teplizumab treatment. This finding suggests there is an active disease window characterized by beta cell stress which may be optimal for administering Teplizumab immunotherapy to delay the onset of stage 3 T1D.
These insights highlight the reality of T1D endotypes and individual differences within T1D, underscoring the need for personalized treatment approaches. Biomarkers of beta cell health can provide valuable insights into the status of beta cell stress, aiding in the development of the most effective treatment strategies for individuals with T1D.
Type 2 Diabetes
T2D is characterized as a metabolic syndrome resulting from the body’s inability to respond effectively to insulin, leading to hyperglycemia. In response to rising blood glucose levels, beta cells initially produce large amounts of insulin, but this prolonged demand for more insulin places significant stress on beta cells. As beta cell function declines, insulin production decreases, and the body can no longer compensate for insulin resistance. This progression results in persistently elevated blood glucose levels and the development of T2D.
Beta cell dysfunction is progressive in T2D, indicating that insulin production deteriorates over time. Consequently, many individuals with T2D will eventually require medications or insulin therapy to manage blood glucose levels effectively.
Fragile beta cells may increase susceptibility to T2D, particularly in the presence of risk factors such as obesity. This suggests that fasting intact proinsulin levels could be analyzed alongside glucose tolerance testing as a potential screening tool for early signs of beta cell dysfunction, helping to predict individuals at risk of developing T2D. Elevated levels of intact proinsulin in the blood indicates beta cell stress and may be predictive of T2D years before clinical symptoms manifest.
While proinsulin has limited efficacy in lowering blood glucose levels, it plays a more significant role in stimulating the differentiation of parenchymal stem cells into pre-adipocytes, which can further differentiate into adipocytes (fat cells). Thus, elevated proinsulin levels are also associated with serious comorbidities such as atherosclerosis and dyslipidemia, due to the effect of proinsulin on pre-adipocytes. This makes increased proinsulin levels both a risk factor and an indicator in T2D.
Islet Cell Transplantation
Islet transplantation is a surgical approach for replacing damaged pancreatic islets in individuals with T1D or chronic pancreatitis, using donor islets to restore insulin production and regulate blood glucose levels. While the procedure offers potential benefits, it also presents challenges, including the need for immunosuppression and moderate long-term graft survival rates.
Several factors influence the success of islet transplantation, including islet mass, graft quality, and autoimmunity. Monitoring transplantation outcomes relies on key biomarkers, such as intact proinsulin, which provide valuable insights into islet function.
Fasting plasma C-peptide measurement is commonly used to assess beta cell function post-transplantation, often integrated into algorithms like BETA-2. However, these approaches have limitations, particularly in their reliance on blood glucose levels, which may not fully reflect islet graft function.
Proinsulin levels are proving to be indicators of graft function and survival. Elevated intact proinsulin levels are typically seen in recipients who require insulin therapy, while stable total proinsulin levels and PI/I (proinsulin-to-insulin) ratios correlate with insulin independence. These findings suggest that impaired insulin processing could serve as an early indicator of graft dysfunction and may help predict insulin dependency after transplantation.
The PI:C ratio is emerging as a promising option for evaluating beta cell dysfunction that could be utilized in islet transplantation studies. Further investigation of PI:C levels could provide insights into graft functionality, potentially leading to enhanced graft preservation and improved patient outcomes.
Conclusion
In conclusion, intact proinsulin is a valuable biomarker for understanding and managing beta cell health in both T1D and T2D, and is showing value as an outcome marker in islet transplantation studies. Its role in identifying early beta cell stress, tracking disease progression, and providing insights into therapeutic windows makes it valuable for improving the diagnosis, treatment, and prevention of diabetes.