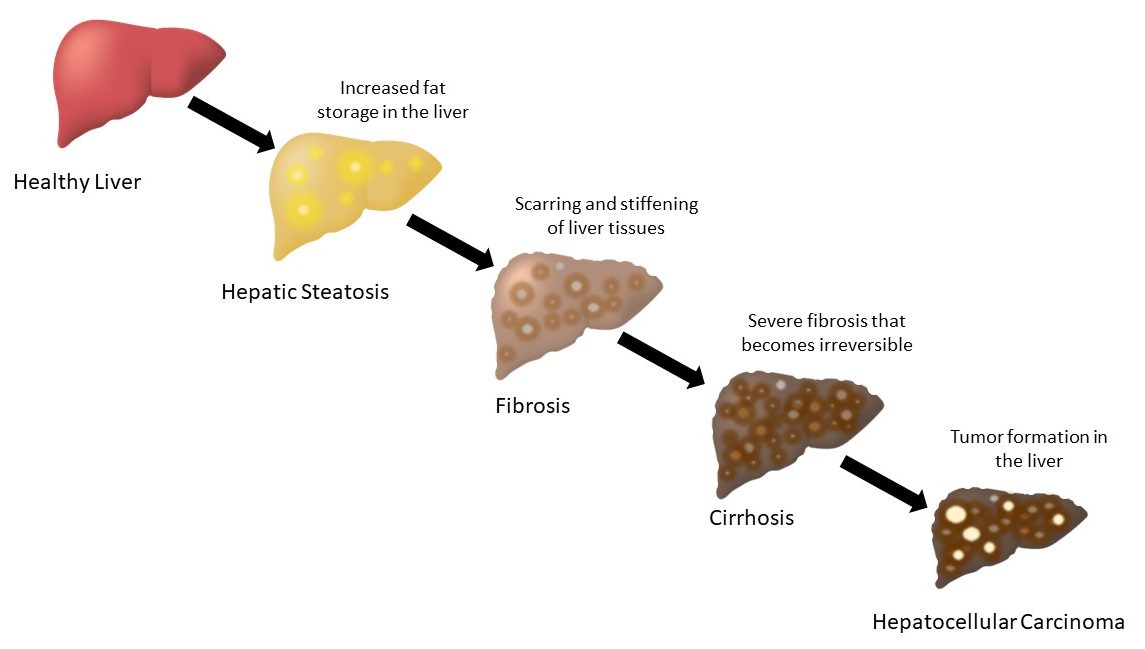
Alcohol-associated liver disease (ALD) is a primary cause of alcohol-related deaths worldwide. ALD is a spectrum of alcohol-driven hepatic disorders that can range from steatosis to hepatitis, fibrosis, and ultimately cirrhosis. Alcohol intake triggers the liver to accelerate fat storage and retention within hepatocytes. Buildup of fat in the liver is called fatty liver disease or hepatic steatosis. With continued excessive alcohol consumption, steatosis can progress into alcohol-associated steatohepatitis (ASH) which is inflammation of the liver. Due to the regenerative properties of the liver, steatosis is reversible following abstinence from alcohol. In lieu of abstinence, steatosis can progress to fibrosis and cirrhosis. Liver fibrosis is the deposition of extracellular matrix proteins, such as collagen, that promote scarring, stiffening of liver tissues, and hepatocyte cell death. Scarred liver tissue is unable to perform normal liver functions and blood flow is inhibited within the liver. Widespread fibrosis impairs liver regeneration, causing in an overall decrease in liver functionality. Cirrhosis is an advanced phase of severe fibrosis that is extensive and often irreversible. When cirrhosis occurs, the liver distorts in shape, shrinks in size, and becomes hard, resulting in irreparable damage that can lead to hepatocellular carcinoma (HCC) liver cancer. Alcohol-associated hepatitis (AH) is a severe form of acute liver inflammation that is associated with high morbidity and mortality.
The liver is the primary location for alcohol (ethanol) metabolism, making it vulnerable to early injury from alcohol intake. Persistent alcohol intake perpetuates ALD through several mechanisms that involve lipid metabolism. Ethanol oxidation enhances the synthesis and storage of lipids in the liver through disruption of normal lipid homeostasis. It does so by slowing down the rate of autophagy in the liver due to inhibited lysosome biogenesis, resulting in an overall loss of lipid catabolism. The liver normally synthesizes very low density lipoprotein (VLDL) to transport triglycerides from the liver to peripheral tissues. However, alcohol impairs lipid export from the liver due to decreased synthesis of intact VLDL. In effect, liver functionality is converted from breaking down lipids to storing lipids during alcohol exposure. These damaging effects of alcohol on lipid metabolism in the liver leads to the accumulation of fat and the development of alcohol-associated steatosis.
Given the complex relationship between alcohol and lipid metabolism in the liver, it is perhaps not surprising that ALD can coincide with other nonalcoholic liver diseases such as nonalcoholic fatty liver disease (NAFLD) and hepatitis C (HCV) infection. NALFD is defined by fat accumulation in the liver and nonalcoholic steatohepatitis (NASH) is a stage of NAFLD that has progressed to include liver inflammation and hepatocyte damage. NAFLD and NASH are largely driven by metabolic complications and obesity. Obesity and alcohol function synergistically to increase the risk of developing liver steatosis and ALD. In fact, genetic polymorphisms in lipid metabolic factors have recently been identified that associate with both NAFLD and ALD. This suggests that lipid metabolism in the liver is a critical component of NASH and ALD pathogenesis.
Diagnosis
ALD is commonly diagnosed following a physical exam looking for enlargement of the liver, accumulation of fluid in the abdominal cavity (ascites), jaundice, and tenderness of the abdomen. During AH diagnosis, ongoing alcohol consumption is considered along with an abstinence period of less than 60 days prior to onset of jaundice. Blood-based lab tests measuring aspartate aminotransferase (AST), and alanine transaminase (ALT), and serum total bilirubin levels are also analyzed during clinical diagnosis.
AH diagnosis can be categorized as definite AH, probable AH, or possible AH. Definite AH diagnosis is achieved through liver biopsy histological analysis and clinical diagnosis. Probable AH is clinically diagnosed without the presence of confounding factors. Possible AH is clinically diagnosed in the presence of confounding factors, such as DILI or ischemic hepatitis. In individuals with possible AH, liver biopsy is the best way to confirm AH diagnoses.
The complexity of ALD and AH is evolving due to western pattern diets, decreases in exercise habits, and contributions of co-morbidities. The common practice of clinical diagnosis based on physical examination has space for improvement in order to better detect and treat the overwhelmed chronic liver disease burden. Liver biopsy histology is the gold standard for determining the type of liver disease, but liver biopsies are invasive, costly, inaccessible, and carry severe risks of bleeding complications and mortality.
Non-invasive methods to diagnose ALD can be carried out with blood-based and imaging-based tests. Blood-based tests are used to measure liver functionality through the assessment of biomarker levels in the serum. Common biomarker indicators of early stages of ALD include gamma glutamyl transpeptidase (GGT),AST, and ALT. GGT is secreted into the bloodstream following excessive alcohol intake or liver injury and serum levels of GGT remain elevated following continued alcohol consumption for several weeks. High GGT levels can indicate liver damage and liver cell death. AST and ALT are traditional biomarkers that are frequently used to assess liver damage and early ALD. Despite their widespread use as liver markers, AST and ALT levels lack specificity and sensitivity to ALD. Carbohydrate deficient transferrin (CDT) is commonly used as a marker of chronic alcohol consumption but may be better suited for determining the severity of liver disease in ALD and non-alcohol-associated liver disease. Advanced ALD is suspected when coagulation factor levels are altered, such as reduced albumin levels, extended prothrombin time and/or international normalized ratio (INR), thrombocytopenia, or elevated bilirubin levels.
Imaging scans non-invasively detect steatosis and fibrosis of the liver, but do not have means of determining the contribution of alcohol to the disease pathogenesis. Transient elastography such as Fibroscan® measures liver stiffness that correlates with stage of fibrosis. It is important to consider the presence of coexisting ASH, inflammation, cholestasis, or hepatic congestion that may increase liver stiffness in ALD patients. Additional imaging techniques include computed tomography (CT) scans, ultrasonography, and magnetic resonance imaging (MRI) that are useful for detecting steatosis, and advanced stages of liver diseases.
Several scoring systems have been developed to characterize the liver disease state and ALD prognosis (Table 1). Static prognostic scores and models such as Maddrey’s discriminant function (MDF or DF), model for end-stage liver disease (MELD), ABIC, and Glasgow alcoholic hepatitis score (GAHS) are commonly used to define AH. DF is widely used to evaluate the benefit and response to corticosteroid therapy in AH individuals. MELD, ABIC, and GAHS scores are used to evaluate mortality risk with AH. GAHS is further leveraged to identify individuals most likely to benefit from corticosteroid treatment and the Lille score monitors response to corticosteroid treatment. These scores do not identify the severity of hepatocyte death nor reflect the pathogenesis of the liver disease, revealing a need for novel biomarkers that probe ALD pathology. Finally, the ALD/NAFLD Index (ANI) is a scoring system that distinguishes ALD from NAFLD with great accuracy.
| Scoring System | Components | Summary |
| ABIC | Age, serum Bilirubin, INR, serum Creatinine | Predicts 90-day survival for alcohol-associated hepatitis. |
| ALD/NAFLD Index (ANI) | AST, ALT, MCV, BMI, gender |
Distinguishes ALD from NAFLD. |
| Child-Turcotte-Pugh score (CTP) | prothrombin time, serum bilirubin, serum albumin, ascites, encephalopathy grade | Determines the severity of cirrhosis and predicts survival. |
| Glasgow alcoholic hepatitis score (GAHS) | Age, serum bilirubin, INR, BUN, WBC | Predicts outcome in alcohol-associated hepatitis and identifies individuals who may benefit from corticosteroid treatment. |
| Lille score | Age, albumin, prothrombin time, Baseline serum bilirubin (Day 0) Change in serum bilirubin (Day 7) | Dynamic score to predict survival rate at 6 months and to advise corticosteroid treatment after 7 days of treatment. |
| Maddrey’s discriminant function (MDF or DF) | prothrombin time, serum bilirubin | Prognostic tool to predict survival and to determine candidacy for corticosteroid or pentoxifylline treatment. |
| Model for end-stage liver disease (MELD) | serum bilirubin, INR, serum creatinine | Prognostic tool to predict short-term survival for alcohol-associated hepatitis and end-stage liver diseases. |
Biomarkers and Research
Biomarkers are powerful biological tools that measure liver function and probe proposed mechanisms involved with ALD pathophysiology. Most importantly, biomarkers provide this information at a non-invasive expense to the subject. Circulating biomarkers are biological components, such as proteins, that can be collected and measured from bodily fluids, such as blood, which offers a highly desired alternative to the invasive standard liver biopsies. In the context of ALD, many biomarkers are being investigated for use in ALD research and clinical trials.
Click here for the full list of ALD and AH related biomarkers available from DiaPharma.
Biomarkers of cell death and regeneration
Cytokeratin 18 (CK18) is a serum biomarker that provides insight into the mechanism of hepatocyte death during ALD. CK18 is an abundant intermediate filament protein expressed in high levels of hepatocyte cytoskeletons and detectable following hepatocyte injury. Following injury to liver cells, CK18 is released into the serum, functioning as a biomarker of cell death. Full length CK18 levels in the serum, measured by the M65® antibodies, could reveal total cell death. The caspase-cleaved CK18 fragment, ccK18, is detectable with the M30® antibody and indicates apoptosis. When both M30® and M65® are analyzed together, the distribution of apoptosis and necrosis can be potentially determined, possibly revealing valuable mechanistic information regarding ALD pathogenesis.
CK18 levels are increased in ALD and correlate with poor disease prognosis and mortality. CK18 better predicted subject mortality compared to the established scoring systems DF and MELD. CK18 also has potential use as a theragnostic biomarker to guide corticosteroid therapy. In addition to detecting hepatocyte cell death, CK18 levels correlate with severe fibrosis in heavy alcohol consumers.
Due to its role as an intermediate filament protein, CK18 is a key component of Mallory-Denk bodies which are characteristic of ongoing inflammation in AH. During AH, hepatocyte ballooning and Mallory-Denk body formation disrupts the cell cytoskeleton, resulting in the release of CK18 filaments. Hence, levels of CK18 are significantly elevated in AH and show great potential for determining the severity of AH, making CK18 an important and unique biomarker. The ratio of CK18/ALT can be used to distinguish AH from other liver diseases, such as NASH, due to necrosis being observed at higher levels in AH compared to NASH. CK18 also has potential to function as biomarkers to predict liver transplant graft success. Serum levels of ccK18 fragments are higher in individuals who lost a liver graft compared to those with graft survivals of greater than 1 year.
WNT3A is a WNT signaling family member that plays a role in liver regeneration. Following liver injury, WNT3A is secreted from Kupffer cells to mediate liver repair pathways. During chronic liver diseases, repeated cycles of cell death and regeneration can lead to fibrosis, cirrhosis, and HCC. Therefore, WNT3A is a promising biomarker to potentially identify chronic liver injury such as HCC, NAFLD, and ALD.
Receptor tyrosine-protein kinase erbB-3 (ERBB3) is a member of the epidermal growth factor receptor (EGFR) family of membrane bound receptors. Hepatocyte ERBB3 signaling is required for the development of liver fibrosis and ERBB3 levels are elevated during HCC. Serum levels of ERBB3 significantly predict the survival of HCV-infected patients with early HCC, suggesting that ERBB3 can function as a prognostic biomarker in this setting. Studies in rodents suggest that miR-148a-3p targets ERBB3 to regulate alcohol-associated liver fibrosis. Additional studies are needed to determine the potential utilization of serum ERBB3 levels as a biomarker for ALD and fibrosis.
Additional liver markers NOGGIN and ASPORIN negatively regulate TGF-β signaling activity during liver regeneration and fibrosis. NOGGIN and ASPORIN levels are significantly decreased during steatosis and NASH. This makes NOGGIN and ASPORIN interesting biomarkers to consider while investigating ALD.
Biomarkers of Immune Response
CD163 is a macrophage receptor protein located on Kupffer cells, the immune macrophage cells residing in the liver. Due to their role as immune first-responders of the liver, Kupffer cells are highly sensitive to changes in the liver. Inflammatory cascades initiated by alcohol metabolism drive the proliferation of Kupffer cells and stimulates the shedding of soluble CD163 (sCD163) from the surface of Kupffer cells. TNF-α cleaves sCD163 from surface of macrophages to regulate inflammation. Elevated levels of sCD163 associate with liver disease severity and poor prognosis.
Lipocalin-2 (LCN2)/NGAL is a carrier protein that is produced during innate immune responses involving inflammation. In addition to being a sensitive biomarker for renal function, serumLCN2/NGAL levels correlate with liver function and LCN2/NGAL levels are elevated in chronic liver diseases. LCN2/NGAL is also a prognostic biomarker that can be used to predict survival in chronic liver diseases, including ALD.
Osteopontin (OPN) is a pro-inflammatory regulator that functions to accelerate the infiltration of immune cells. OPN is normally expressed in the bile duct epithelium, but OPN expression can become activated in hepatic stellate cells (HSCs) to promote liver regeneration following liver injury. OPN overexpression can become problematic due to its role as a mediator of inflammation, such that elevated OPN expression leads to fibrosis and scarring. Increased serum levels of OPN strongly correlate with severe liver fibrosis in DILI, NASH, and ALD. This makes OPN an important liver fibrosis and inflammatory biomarker for the investigation of ALD and chronic liver diseases.
Complement activation is an important part of the innate immune system and the majority of complement components are produced in the liver. The complement system is activated during multiples stages of ALD, such as alcohol-associated steatosis, AH, and cirrhosis. The alcohol metabolite acetaldehyde drives the activation of complement protein C3. Serum levels of C3a is associated with steatosis and liver injury following chronic alcohol use. On the other hand, complement component C5 appears to have a protective function against lipid accumulation in the liver. Complement activation is a diagnostic and prognostic biomarker for individuals with AH. More research is needed to understand the mechanisms of complement function during ALD and AH.
ST2 receptor is a receptor that binds the cytokine interleukin-33 (IL-33) ligand. IL-33 is released from damaged and necrotic cells. Upon IL-33/ST2 receptor binding, an inflammatory cascade is initiated that is linked to hepatic fibrosis and inflammation. The ST2 receptor has potential use as a diagnostic biomarker for the determination of liver inflammation. The ratio of IL-33/ST2 receptor could be evaluated as an indicator of ALD severity.
Circulating small non-coding RNA (miRNA) have shown promise as ALD biomarkers due to their role as posttranscriptional regulators over a diverse range of liver functions. In addition to being localized within cells, miRNAs can also be detected in the serum, saliva, and urine. miR-122 is found in hepatocytes and is thought to be released into the serum following hepatocyte injury. Hence, elevated miR-122 levels in the serum indicate hepatocyte damage making miR-122 an interesting biomarker for chronic liver diseases such as ALD, NASH, and drug-induced liver injury (DILI). Additional miRNAs that have biomarker utility include miR-192 and miR-30a that are found in high levels of exosomes during AH. miR-155 promotes liver injury in ALD. When miR-155 levels are deficient, neutrophil infiltration is reduced and the effects of alcohol-induced steatosis and oxidative stress are decreased. Long-non-coding RNAs (lncRNAs) AK128652 and AK054921 have also shown increased expression in the serum of individuals with alcohol-associated cirrhosis.
Therapeutics
Current ALD Therapies
There are currently no targeted drugs available to treat ALD. The best treatment for ALD is abstinence from alcohol. The liver has regenerative capabilities that can occur when chronic alcohol exposure is removed. Studies have shown that alcohol-associated steatosis can resolve, and survival rates of cirrhosis can improve when abstinence is observed. Therapeutics are available to help maintain sobriety, but these drugs are not approved for the treatment of ALD. Treatment for alcohol use disorder (AUD) may help to support abstinence during the course of ALD therapies and liver transplantation.
Corticosteroids have shown benefit for reducing inflammation in ALD, although 40% of ALD patients are unresponsive to corticosteroid therapies. Individuals with active infection, such as chronic hepatitis, should avoid corticosteroid therapies because complications such as sepsis could develop following steroid treatment.
Pentoxifylline (PTX) is an indirect inhibitor of the proinflammatory cytokine tumor necrosis factor (TNF) and can be used as a replacement for steroid therapies. PTX has anti-fibrotic properties and reduces the secretion of collagen in the liver.
Nutritional support is critical for treating malnourishment in individuals with ALD to prevent the development of infections.
Liver transplantation is the best therapeutic option in advanced stages of ALD that are unresponsive to corticosteroid therapies, such as cirrhosis and HCC. There are ethical factors to consider surrounding the use of liver transplantation for ALD due to the high incidence of alcoholic relapse (10%-50%) following transplantation. Liver transplant recipients have a greater risk of developing cardiovascular complications and de novo cancer, perhaps due to effects of immunosuppressive drugs and other lifestyle factors such as smoking.
The Future of ALD Therapy
New ALD treatment options are being investigated to address the pathophysiology of ALD.
Hepatocyte apoptosis is a leading feature of chronic liver diseases. Apoptosis inhibitors, such as caspase inhibitors, have shown efficacy in reducing fibrosis and liver injury in HCV and NASH clinical trials. Given that hepatocyte apoptosis is prominent in ALD, there is great potential for apoptosis inhibitors during the treatment of ALD. Further studies are needed to explore this avenue.
Chemokines and interleukins play a role in the pathogenesis of ALD and liver inflammation. Chemokines and interleukins facilitate the recruitment and infiltration of neutrophils and inflammatory factors, which promote liver damage. Chemokines and interleukin levels are elevated in ASH livers and correlate with prognosis. ALD therapies that target chemokines and interleukins, such as anti-TNF-α agents and IL-22 (F-652), are under investigation.
Epigenetic regulation of DNA methylation is being investigated for its efficacy in treating liver diseases, including AH. Through binding and inhibiting DNA methyltransferase activities, DUR-928 regulates the expression of genes that are involved with cell death, inflammation, and liver regeneration. Clinical Phase 2a data showed a reduction in bilirubin levels, suggesting that DUR-928 may be an effective new therapy for AH.
Oxidative stress is a target under investigation for ALD treatment. S-adenosylmethionine (SAM) has antioxidant properties and is a methyl donor that is required for normal liver functions. Alcohol is a disruptor of methionine and oxidative reactions, and therefore SAM levels are decreased in ALD. Early clinical trials have shown potential for treatment with SAM to improve alcohol-associated cirrhosis survival rates, although a study analyzing 24-week treatment with SAM did not improve ALD outcomes. It is possible that a longer-term of SAM treatment may be more effective at treating ALD. Betaine synthesizes SAM through the methylation of the SAM-precursor, methionine. Betaine protects the liver from injury, prevents alcohol-induced steatosis, apoptosis, and oxidative stress. Further studies are needed to investigate the clinical efficacy of SAM and Betaine to treat ALD. Omega 5 fatty acid antioxidant is being evaluated in individuals with severe AH.
Early clinical studies suggest that stem cell transplantation reduces liver inflammation, ameliorates fibrosis, and improves liver functionality when administered to individuals with liver cirrhosis.
Combination therapies are being exploring using the immunosuppressant drug mycophenolate mofetil (MMF), particularly in severe AH populations that are unresponsive to steroids
Treatments that target AUD are under investigation for efficacy for treating ALD. Metadoxine (MTD) is approved in Europe, but not in the USA, to accelerate the elimination of alcohol from the bloodstream. Clinical trial data suggests that administration of MTD improves liver functionality tests, promotes abstinence, and increases survival rates in ASH subjects.
Alcohol ingestion alters gut microflora, leading to intestinal permeability. This allows the entrance of bacterial antigens and toxins into the circulation and liver. To target intestinal permeability and the gut-liver axis, probiotics are being investigated to restore gut microflora in ALD. Likewise, antibiotics such as rifaximin are being considered to inhibit the growth of toxic bacteria that cause hepatic encephalopathy in ALD.