Type 2 Diabetes and MASH: Unraveling the Metabolic Crosstalk
Posted on: December 10, 2024
-Contributed by Olivia Stricker, PhD and Abi Kasberg, PhD
The relationship between metabolic disorders and liver disease is striking. Liver disease affects 75% of individuals with type 2 diabetes (T2D), making metabolic disorders the most common underlying cause of liver disease in the U.S (Gobejishvili et al. 2024). The liver diseases associated with T2D range from metabolic dysfunction-associated steatosis liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH) to cirrhosis and hepatocellular carcinoma (HCC) (Gobejishvili et al. 2024). Thus, T2D is a significant risk factor of liver disease progression and can accelerate liver disease severity.
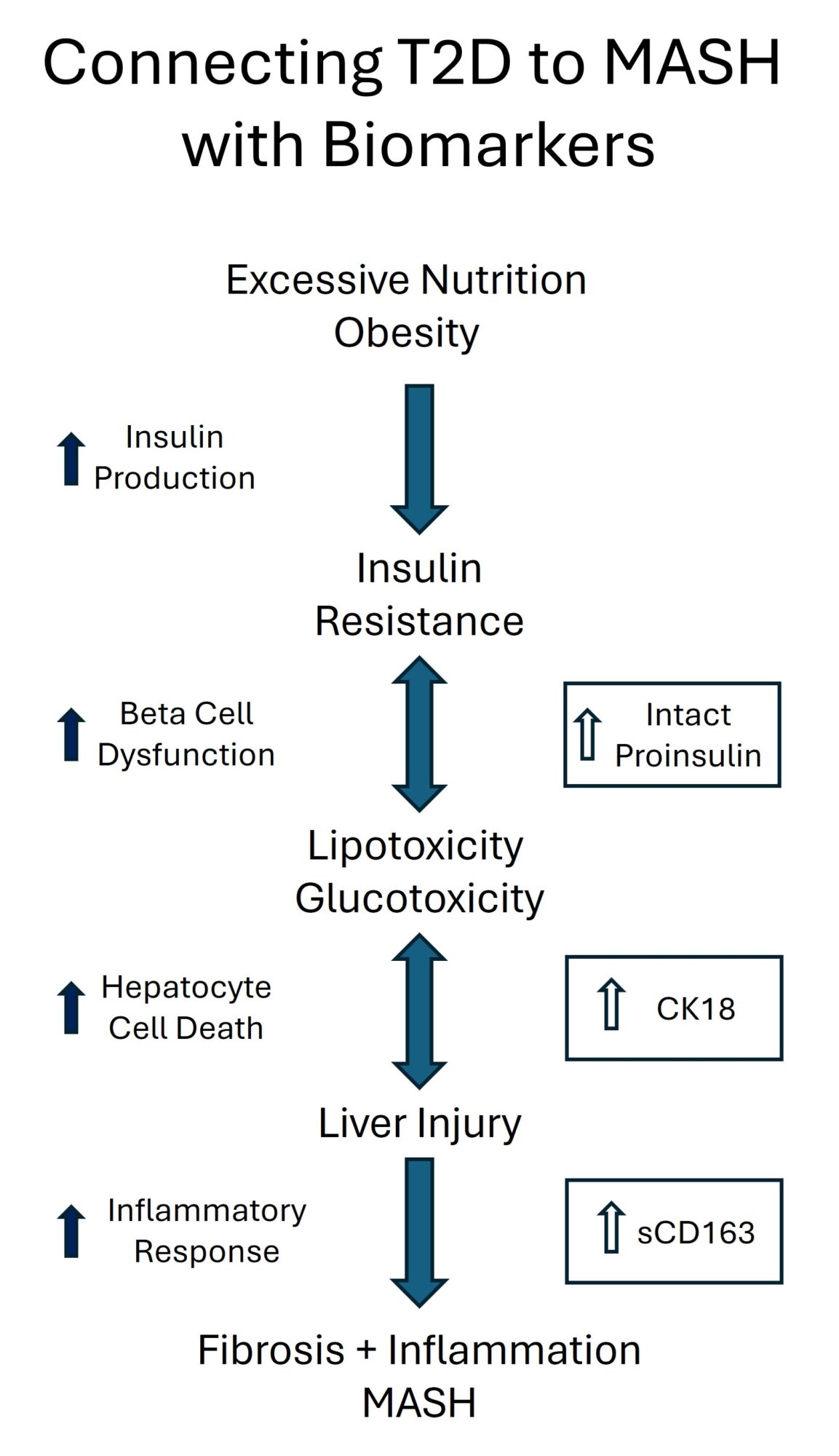
Insulin production, beta cell dysfunction, and the development of MASH are interconnected through a complex metabolic and inflammatory network that involves both the pancreas (where insulin is produced), and the liver (where MASH occurs), highlighting the pathological crosstalk between the two organs. Investigating these connections using biomarkers, like intact proinsulin, and indicators of hepatocyte apoptosis, like caspase-cleaved cytokeratin 18 (CK18), can provide valuable insights into the pathophysiology of these metabolic conditions.
How is pancreatic insulin production connected to liver disease?
Insulin Resistance and Hyperinsulinemia:
Insulin is a hormone that facilitates the uptake of glucose into cells for energy. A hallmark characteristic of metabolic syndrome and T2D is insulin resistance, a condition where the body is unable to respond to insulin. The effects of insulin resistance are two-fold. First, hyperglycemia occurs, which is the elevation of blood glucose levels. Secondly, hyperglycemia causes an increased demand on pancreatic beta cells to produce more insulin to compensate for the rising blood glucose levels. The increased production and secretion of insulin is called hyperinsulinemia. Compensatory hyperinsulinemia, together with glucotoxicity, caused by high levels of blood glucose, can damage beta cells and inhibit their functional capacities.
Impact on the Pancreatic Beta Cell:
Beta Cell Dysfunction: As the beta cells become overburdened and damaged, they begin to lose their capacity to produce insulin effectively. When insulin is not produced or processed properly, its intermediate form intact proinsulin is secreted at increased levels into the bloodstream. Elevated levels of intact proinsulin are indicative of beta cell stress and dysfunction (Pfützner et al. 2004). Thus, elevated levels of intact proinsulin are often seen in individuals with prediabetes and can function as an early risk indicator for those likely to progress to T2D within 4 years or more (Pfützner et al. 2015). It has been further suggested that fragile beta cells may predispose individuals to T2D and the damaging effects of insulin resistance (Ikegami et al. 2021).
Lipotoxicity and Inflammation: In addition to the damaging effects of glucotoxicity, lipotoxicity is also harmful to beta cells (Vilas-Boas et al. 2021). Prolonged exposure to lipids, such as during obesity or metabolic syndrome, can cause fat buildup in beta cells in the form of triglycerides (Al-Mrabeh 2021). This fat buildup disrupts normal cellular functions, leading to metabolic stress within the beta cells. Lipotoxicity also triggers inflammatory pathways and the production of pro-inflammatory cytokines which leads to beta cell dysfunction or cell death. The metabolic and immune responses triggered by beta cell dysfunction and hyperglycemia can activate inflammatory pathways, contributing to hepatocyte injury and progression from steatosis to steatohepatitis (MASH) (Habib 2024).
Impact on the Liver:
Lipid Accumulation: The liver plays a central role in regulating glucose, lipid, and insulin metabolism. In parallel to the effects on pancreatic beta cells, hyperinsulinemia and insulin resistance drive lipid accumulation in the liver (hepatic steatosis) and hepatic inflammation, contributing to the progression of MASH (Steneberg et al 2015). In T2D, increased adiposity is linked to dysregulated release of adipokines such as adiponectin and leptin by white adipose tissue (He et al. 2024, Vilarino-Garcia et al. 2024). White adipose tissue dysfunction and increased lipolysis due to insulin resistance result in elevated free fatty acid accumulation in the liver, which can cause hepatocyte stress and liver injury (Bansal et al. 2024).
Hyperglycemia and Gluconeogenesis: The liver stores excess glucose as glycogen, but when glycogen stores are saturated, excess glucose is diverted into lipid synthesis pathways, leading to increased fat production (lipogenesis). Continuous hyperglycemia causes glucose to be converted into fatty acids and triglycerides, a process known as De Novo lipogenesis, which promotes steatosis and MASLD. During insulin resistance, the liver also increases gluconeogenesis, producing glucose from non-carbohydrate sources. This further exacerbates hyperglycemia and enhances lipid storage, worsening fatty liver disease. Glucose-induced oxidative stress and endoplasmic reticulum stress ultimately lead to apoptosis in the liver (Hayashi et al. 2024).
Inflammation and Apoptosis: The accumulation of excess glucose and fatty acids due to insulin resistance can cause lipotoxicity and glucotoxicity, which promote inflammation and apoptosis in liver cells, driving the progression of fatty liver disease and liver damage. Intestinal barrier dysfunction and systemic inflammation drive pathological changes to the gut-liver axis, contributing to hepatocyte inflammation and liver injury during MASH and T2D (Gobejishvili et al. 2024).
Crosstalk Between the Pancreas and the Liver:
Pro-inflammatory cytokines and adipokines produced during beta cell dysfunction and liver inflammation can create a harmful feedback loop that exacerbates both insulin resistance and liver damage. Beta cell dysfunction increases cytokine production, which further impairs insulin sensitivity and exacerbates liver inflammation. In turn, liver inflammation stimulates the release of adipokines that can aggravate beta cell function and worsen insulin resistance. This cyclical interaction highlights the intricate connection between metabolic and inflammatory pathways, driving metabolic conditions like T2D and MASH.
Biomarkers For Understanding the Metabolic Connection of T2D and MASH
- Intact Proinsulin as a Biomarker of Beta Cell Dysfunction:
- Elevated intact proinsulin levels can serve as a biomarker of early beta cell dysfunction. This can be particularly useful in research aiming to identify individuals at risk of developing MASH or T2D due to insulin resistance.
- Studying intact proinsulin levels in conjunction with other markers of insulin resistance, such as glucose tolerance testing and C-peptide levels, can help identify the transition from beta cell compensation to beta cell failure.
- The ratio of proinsulin to C-peptide, PI:C, has been used to assess beta cell dysfunction in diabetes drug development studies and clinical trials. The PI:C ratio has been shown to associate with prolonged hyperglycemic time in T2D (Miya et al. 2024).
- CK18 as a Biomarker of Liver Apoptosis, Inflammation, and Damage:
- Hepatocyte apoptosis (programmed cell death) is a key feature of liver damage in MASH. Measuring biomarkers of apoptosis, such as caspase-cleaved cytokeratin-18 (CK-18), can provide insight into the severity of liver inflammation and damage caused by glucotoxicity, lipotoxicity, and other mediators of liver injury.
- The level of hepatocyte apoptosis may be linked to insulin resistance and beta cell dysfunction, establishing a connection between pancreatic endocrine function and liver pathology.
- Inflammatory Signaling Receptors as Biomarkers of Gut-Barrier Dysfunction:
- CK18 levels correlate with inflammatory biomarkers sCD14 and sCD163, suggesting that immune cell activation and hepatic inflammation may be linked to the development of liver injury in T2D. Pathogenic changes in the gut-liver axis, marked by increased microbial translocation, may be a major component in the etiology of hepatocyte inflammation and injury in patients with T2D (Gobejishvili et al. 2024).
How to Use these Biomarkers to Explore the Interplay of Organ Contributors to Metabolic Disorders
- Simultaneous Measurement of Intact Proinsulin and Apoptotic Markers:
- Measure intact proinsulin in plasma as an indicator of beta cell stress.
- Assess hepatocyte apoptosis and liver injury by measuring serum levels of CK18 fragments or other liver apoptosis biomarkers.
- Longitudinal Studies:
- Track changes in beta cell dysfunction, intact proinsulin levels, insulin resistance, and liver damage over time.
- Correlate biomarker changes with clinical outcomes, such as progression from simple steatosis to MASH.
- Correlation Analysis:
- Analyze the relationships between intact proinsulin, apoptosis markers, and other metabolic parameters (e.g., fasting glucose, HbA1c, lipid profiles) to explore connections between beta cell health and liver pathology.
- Interventional Studies:
- Evaluate how lifestyle interventions or medication affect intact proinsulin and apoptosis markers to determine their impact on beta cell function and MASH progression.
Drug Development and Cross-Organ Impacts
Given the connection between the pancreas and the liver in metabolic disorders, drugs approved for treating type 2 diabetes (T2D) are under investigation for their effectiveness in managing MASH and liver injury (Table 1). Likewise, it would be interesting to determine whether Resmetirom, the first FDA-approved treatment for adults with MASH and liver fibrosis, demonstrates efficacy in treating T2D.
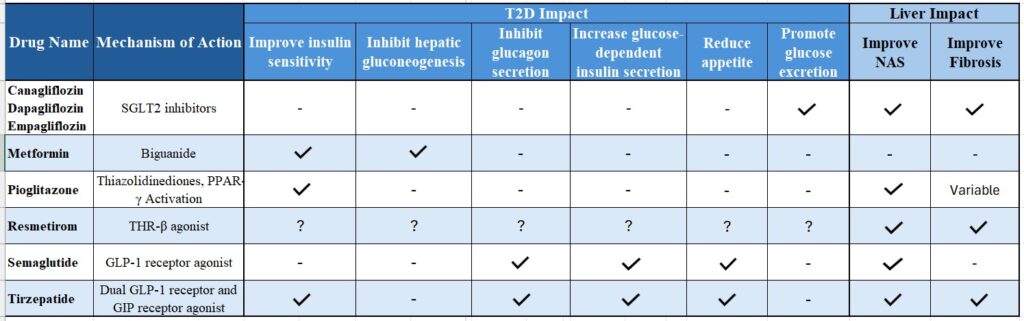
Table 1: Approved therapeutics for the treatment of T2D have shown positive effects on liver health, as evidenced by improvements in liver injury assessed through the NAFLD Activity Score (NAS) and reductions in liver fibrosis in clinical research studies, as indicated. Resmetirom has received FDA approval to treat MASH and its efficacy in treating T2D remains unknown.
Conclusion
Intact proinsulin and biomarkers of hepatocyte apoptosis provide valuable insights into the connection between beta cell dysfunction and the progression of MASH. Focusing on these biomarkers enables researchers to better understand how disruptions in insulin production and beta cell function contribute to liver disease, facilitating the development of targeted therapies for metabolic disorders. This complex interplay between insulin resistance, hyperinsulinemia, lipotoxicity and multi-organ crosstalk plays a pivotal role in driving both T2D and MASH, making this an essential area of study.
Further Reading:
Al-Mrabeh, A. (2021). Β-cell dysfunction, hepatic lipid metabolism, and cardiovascular health in type 2 diabetes: New directions of research and novel therapeutic strategies. Biomedicines, 9(2), 226. https://doi.org/10.3390/biomedicines9020226
Bansal, S. K., & Bansal, M. B. (2024). Pathogenesis of MASLD and MASH – role of insulin resistance and lipotoxicity. Alimentary Pharmacology & Therapeutics, 59(S1). https://doi.org/10.1111/apt.17930
Gobejishvili, L., Vatsalya, V., Avila, D. V., Feygin, Y. B., McClain, C. J., Mokshagundam, S., & Barve, S. (2024). Association of circulating markers of microbial translocation and hepatic inflammation with liver injury in patients with type 2 diabetes. Biomedicines, 12(6), 1227. https://doi.org/10.3390/biomedicines12061227
Habib, S. (2024). Team players in the pathogenesis of metabolic dysfunctions-associated steatotic liver disease: The basis of development of pharmacotherapy. World Journal of Gastrointestinal Pathophysiology, 15(4), 93606. https://doi.org/10.4291/wjgp.v15.i4.93606
Hayashi, T., Oe, S., Miyagawa, K., Kusanaga, M., Ogino, N., Honma, Y., & Harada, M. (2024). Excess glucose alone induces hepatocyte damage due to oxidative stress and endoplasmic reticulum stress. Experimental Cell Research, 442(2), 114264. https://doi.org/10.1016/j.yexcr.2024.114264
He, L., Xuan, W., Liu, D., Zhong, J., Luo, H., Cui, H., Zhang, X., & Chen, W. (2024). The role of adiponectin in the association between abdominal obesity and type 2 diabetes: A mediation analysis among 232,438 Chinese participants. Frontiers in Endocrinology, 15, 1327716. https://doi.org/10.3389/fendo.2024.1327716
Ikegami, H., Babaya, N., & Noso, S. (2021). β‐Cell failure in diabetes: Common susceptibility and mechanisms shared between type 1 and type 2 diabetes. Journal of Diabetes Investigation, 12(9), 1526–1539. https://doi.org/10.1111/jdi.13576
Miya, A., Nakamura, A., Nomoto, H., Kameda, H., & Atsumi, T. (2024). Positive association between the proinsulin-to-C-peptide ratio and prolonged hyperglycemic time in type 2 diabetes. Endocrine Journal, 71(4), 403–408. https://doi.org/10.1507/endocrj.EJ23-0525
Pfützner, A., Hermanns, I., Ramljak, S., Demircik, F., Pfützner, A. H., Kann, P. H., & Weber, M. M. (2015). Elevated intact proinsulin levels during an oral glucose challenge indicate progressive ß-cell dysfunction and may be predictive for development of type 2 diabetes. Journal of Diabetes Science and Technology, 9(6), 1307–1312. https://doi.org/10.1177/1932296815607862
Pfützner, A., Kann, P. H., Pfützner, A. H., Kunt, T., Larbig, M., Weber, M. M., & Forst, T. (2004). Intact and total proinsulin: New aspects for diagnosis and treatment of type 2 diabetes mellitus and insulin resistance. Clinical Laboratory, 50(9–10), 567–573.
Steneberg, P., Sykaras, A. G., Backlund, F., Straseviciene, J., Söderström, I., & Edlund, H. (2015). Hyperinsulinemia enhances hepatic expression of the fatty acid transporter cd36 and provokes hepatosteatosis and hepatic insulin resistance. The Journal of Biological Chemistry, 290(31), 19034–19043. https://doi.org/10.1074/jbc.M115.640292
Vilariño-García, T., Polonio-González, M., Pérez-Pérez, A., Ribalta, J., Arrieta, F., Aguilar, M., Obaya, J., Gimeno-Orna, J., Iglesias, P., Navarro, J., Durán, S., Pedro-Botet, J., & Sánchez-Margalet, V. (2024). Role of leptin in obesity, cardiovascular disease, and type 2 diabetes. International Journal of Molecular Sciences, 25(4), 2338. https://doi.org/10.3390/ijms25042338
Vilas-Boas, E. A., Almeida, D. C., Roma, L. P., Ortis, F., & Carpinelli, A. R. (2021). Lipotoxicity and β-cell failure in type 2 diabetes: Oxidative stress linked to nadph oxidase and er stress. Cells, 10(12), 3328. https://doi.org/10.3390/cells10123328