The Debate of Early-Liver Transplantation for Alcohol-associated Liver Diseases
Posted on: December 21, 2022
-Contributed by Abi Kasberg, PhD
After recently attending the AASLD Emerging Topics in Alcohol-associated Liver Disease conference, it quickly came to my attention the complexities and challenges that are faced while treating alcohol- associated liver diseases (ALD).
For one, current treatment options for ALD are incredibly limited. ALD therapies are disputed in effectiveness and can vary from institution to institution. In most cases of acute alcohol-associated hepatitis (AH), liver transplantation is the best treatment option available. When allocating liver transplants amongst liver disease candidates, it is important to stratify the severity of liver disease in order to prioritize liver transplants. For reasons unknown, some liver disease patients will recover spontaneously while others will deteriorate without a liver transplant. It remains a mere speculation on who will recover and who will not. Several of the scoring systems used to determine liver disease severity and liver transplant priorities were developed using chronic liver disease populations, not acute disease populations. This means that scores such as the model for end stage liver disease (MELD) may not accurately reflect the severity of acute liver diseases compared to chronic liver diseases.
“Early” liver transplantation, which is the practice of granting liver transplants without the requirement of 6 months of abstinence, is changing the landscape of liver transplantation practices nationwide. It is driving important conversations surrounding the allocation of this scarce resource. How should fairness and ethicality play a role in the transplantation selection process? Who should receive expedited transplants while others must wait?
Meanwhile, the transplantation process is not fully transparent with patients. There is a strong influence of non-liver factors that impact candidacy for liver transplantation. This includes things like strength of familial support systems, law-breaking behaviors, regional discrepancies, and more. Psychosocial evaluations encourage equity among transplant candidates and function to detect candidates who may be at risk for adverse outcomes before and after transplantation (Matthews and Lucey 2022). However, many patients with acute AH receive medical care while being in a reduced state of consciousness and are unable to undergo a full psychiatric evaluation. In some cases, breach of a previously signed abstinence contract may even be grounds for removal from the transplant waitlist, forever.
Alcohol-use disorder (AUD) treatment is typically a low-priority treatment avenue for ALD patients. Hepatology providers are generally not comfortable discussing AUD or prescribing AUD medication. Thus, many hepatologists will not see patients with ALD until they have achieved a designated period of abstinence. This has resulted in a lack of continuity in medical services and a deficiency in substance abuse support for a community in which abstinence is extremely important for survival.
Here is a summary of what I learned, the careful data, thoughtful insights, and important discussions that captured my attention while in attendance at the 2022 ALD Emerging Topics conference.
ALD Epidemiology and Treatment
Alcohol use, and thus ALD rates, are rapidly rising worldwide particularly in young populations in the age ranges of 15-44 years old (Tapper and Parikh 2018). The global burden of alcohol-related deaths is approximately 5% of all deaths (WHO 2022). The COVID-19 pandemic has been a significant driver of alcohol use, along with ease of access to alcohol and barriers to healthcare. Alcohol-related liver diseases have become a major source of healthcare and economic costs.
Despite its impact, there are surprisingly few treatment options to offer patients. Practice guidelines recommend utilizing prednisolone (corticosteroid), antioxidants, and nutrition to treat acute AH, but there is disagreement regarding the best utility of these therapeutics. There is a golden window of time to initiate corticosteroid treatment for patients with acute AH. However, 40-50% of severe AH patients will not respond to corticosteroids, making the utility of corticosteroid therapy inconsistent (Singal et al. 2011). At best, there is an increase of 30-day survival rates in steroid-responders (Arab et al. 2021). Even so, it is important to identify who will respond to corticosteroids and who will not. For instance, steroids can be detrimental for some patients who have undetected or low levels of bacterial infections. Steroid use in these instances could lead to a worsening of prognosis. Corticosteroid treatment also appears to be ineffective for the treatment of extremely severe liver disease, such as cirrhosis. Scores that can be used to predict response to treatment, the Lille score and the MELD score, fall short in determining individualized treatment courses or accounting for disease specificity.
There are little more than a few specks on the horizon for novel ALD treatment options. Interleukin 22 (IL-22) has antioxidant, anti-microbial, and anti-apoptotic properties that are being investigated for therapeutic potential to treat inflammatory diseases. The utility of a recombinant fusion protein containing interleukin-22 (IL-22) and immunoglobulin G2 (IgG2), named F-652, is under development for the treatment of acute AH and graft vs host disease (Tang et al. 2019). The epigenetic regulator DUR-928 is also being studied for its role in regulating the expression of genes that control liver cell death and regeneration (Clinical trials #: NCT03917407).
|
Updated ALD Terminology Guidelines To reduce the significant weight of stigma that accompanies ALD, the following changes in terminology have been recommended by the AASLD and hepatology community: |
|
| Previous Term | Current Term |
| Alcoholism / Alcoholic | Alcohol use disorder (AUD) |
| Alcoholic cirrhosis (AC) | Alcohol-associated cirrhosis (AC) |
| Alcoholic liver disease (ALD) | Alcohol-associated liver disease (ALD) |
| Alcoholic hepatitis (AH) | Alcohol-associated hepatitis (AH) |
| Alcoholic steatohepatitis (ASH) | Alcohol-associated steatohepatitis (ASH) |
| Sobriety | Abstinence |
Liver Transplantation
Early liver transplantation is often the best option for survival in individuals with acute AH (Lee et al. 2019, Cholankeril and Ahmed 2018). Despite this, there is a disparity in the liver transplantation approval rate for patients with ALD. Patients with ALD made up 30% of the liver transplant waitlist in the United States in 2016, however less than a quarter (24%) of patients with ALD received liver transplants (Cholankeril and Ahmed 2018). This disparity is further amplified by race and sex. Among individuals with ALD, women and black populations have the lowest access to liver transplants (Kaplan et al. 2022, McElroy et al. 2020). Recently, a broader recognition of ALD as an indication for liver transplantation has led to it being the leading indication for liver transplantation. Still, more work needs to be done to understand and address the inequities of ALD and access to liver transplantation.
The weight of MELD scores
The MELD score predicts mortality within a time frame of 90 days for liver disease patients. MELD scores carry considerable leverage in determining access to and priority of liver transplants. Additional factors such as co-morbidities, psychosocial considerations, and additional lab work are always considered in addition to MELD scores, but it appears that MELD ≥ 21 is a standard prerequisite for liver transplantation consideration. Generally speaking, the assumption is that the higher the MELD score, the greater the chance for 90-day mortality, and the more urgent the need for liver transplantation.
Typically, acute AH patients are sicker and have higher MELD scores than chronic liver disease patients. Despite this, AH patients are most likely to be declined for liver transplantation due to psychosocial factors such as lack of support systems, concerns about home environments, law-breaking behaviors, substance abuse, and mental health conditions.
It is important to mention that due to the impact of MELD scores in prioritizing need for liver transplantation, chronic liver diseases with low listing MELD scores are rarely allocated a liver transplant. Patients with low MELD scores make up a majority of the waitlist (71% in 2015) yet remain at significant risk of death due to waitlist dropout or death from liver and non-liver-related causes instead of receiving liver transplants (Kwong et al. 2016). It may even seem contradictory that a rapid increase of MELD score (5 points within 30 days) represents a decompensating event that excludes patients from liver transplantation, instead of prioritizing them as an increased need for liver transplantation (Kwong et al. 2016). This has created a demand for novel disease-specific indicators to differentiate liver diseases, accurately determine liver disease severity, and improve the selection of liver transplantations.
Flow of care
The standard flow of care for an ALD/AH patient begins with being seen by a primary care provider (PCP) or emergency care provider. The PCP analyzes standard liver tests (ALT, AST, bilirubin, and more) to determine if liver injury has occurred. If so, the patient may be referred to a hepatologist (Figure 1). Due to a limited supply of hepatologists, some medical networks require a period of abstinence before an ALD patient may receive medical care from a hepatologist. Therefore, not all hepatologists provide service to actively-drinking ALD patients. This can create a barrier to care, as patients must be referred to transplant centers, typically through hepatologists, prior to being placed on a waitlist for liver transplantation (Volk et al. 2011). There are approximately 140 transplant centers in the United States. Every transplant center has its own protocols, committees, and procedures. This has created a nationwide lack of standardization nor consistency in protocols for the allocation of liver transplants.
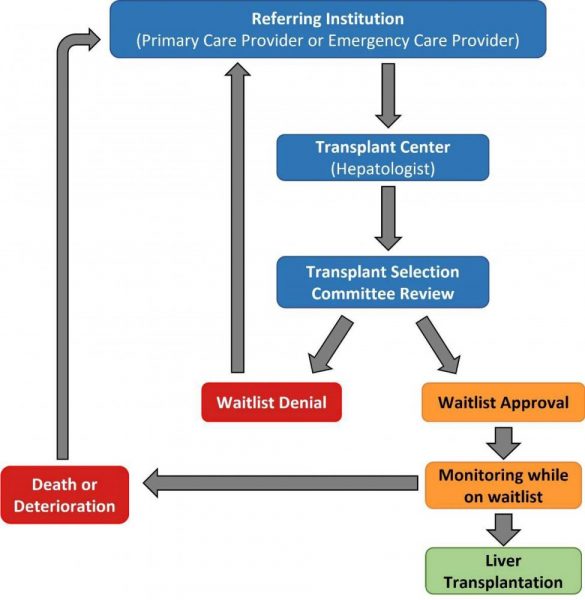
Figure 1: Flow of care for patients with alcohol-associated liver disease or acute alcohol-associated hepatitis. Figure adapted from Millson et al. 2020.
Transplant selection committee reviews
When liver transplantation has been determined to be the remaining and best course of treatment, acute AH cases are funneled to transplant centers. In 2020, over 50,000 patients died of chronic liver disease and cirrhosis in the United States, 24,900 candidates were waitlisted for liver transplantation, and 8,906 liver transplants were performed (HRSA 2020). Needless to say, liver organ supplies are limited.
The purpose of liver transplantation selection committees is to determine candidacy and fair allocation of this scarce resource. Multidisciplinary liver transplantation selection committees review patient medical records to determine placement on the waitlist (Figure 1). This may include confirmation of the diagnosis, verifying that medical treatment has been considered, and evaluating comorbidities and contraindications (Millson et al. 2020). The structure of liver transplantation committee meetings and criteria for candidate selection vary by transplant center. The decisions made by the selection committees are heavy, highly discussed, and always well-intentioned.
|
Who is on a Liver Transplant Selection Committee? Liver transplant selection committees are consistently composed of hepatologists, liver transplant surgeons, social workers, and transplant coordinators (Volk et al. 2011). Additional members of the committee may include, with variability amongst transplant centers, neuropsychologists, addiction specialists, and finance experts. |
When possible, liver transplantation selection committee members individually meet with patients prior to committee meeting discussion. In a closed committee meeting format, patients’ medical histories are reviewed along with psychosocial, substance abuse, and financial concerns (Volk et al. 2011). The goal of these meetings is to identify possible reasons for exclusion of liver transplantation eligibility. The decision-making process is considered to be democratic, with some centers facilitating formal voting while other centers do not. There are many multi-dimensional layers of preexisting co-morbidities and psychosocial influences that go beyond MELD scores to impact liver transplant consideration.
Shifts in abstinence protocols prior to liver transplantation
Until recently, most transplant centers in the United States required a period of 6 months of abstinence prior to liver transplantation for ALD candidates (Lee et al. 2019). The reasoning behind a 6-month period of abstinence, termed the “6-month rule”, was to give the injured liver time to recover in order to avoid liver transplantation (Lee et al. 2018). In actuality, the 6-month rule is not realistic for most severe AH patients, who have by AH definition, recently or are actively consuming alcohol. Also, up to 90% of deaths occur within 2 months of AH diagnosis, making the 6-month rule an improbable and arguably an inhumane barrier to transplantation (Lee et al. 2018, Obed et al. 2015). 6 months of abstinence pre-liver transplant does not predict the risk of relapse post-liver transplant, making it an ineffective tool at predicting post-transplant abstinence (Rice and Lucey 2013).
Thus, the 6-month rule has largely been removed from standard practice in order to best support the survival outcomes of patients with acute AH. In its place, early-liver transplantation is being considered for acute AH patients. Shortening the period of abstinence enables more patients with acute AH to survive long enough to receive a liver transplant (Lee et al. 2019). This shift in protocol has created important discussions surrounding abstinence prior to liver transplantation: Should a period of abstinence be required of patients with ALD prior to liver transplantation? If so, how long should the duration be?
Early liver transplantation
Early liver transplantation is when liver transplantation occurs in patients with ALD without requiring the 6-month rule of abstinence. Early liver transplantation has been shown to be beneficial for severe AH patients in achieving survival at 1-year (94%) and 3-years (84%) post-transplant (Lee et al. 2018). In contrast, survival rates without liver transplantation in severe AH patients were 10-30% at 1 year (Kwon et al. 2021). Further analysis needs to be undertaken to fully investigate the dynamic outcomes of liver transplantation for ALD.
The greatest medical concerns following early-liver transplantation are sepsis and post-liver transplant alcohol use. Therefore, an important strategy to provide effective support to individuals with AH following liver transplantation is to integrate AUD therapy at transplant centers and minimize barriers to AUD therapy. The timely identification of post-transplant alcohol use combined with effective interventions would be important steps towards avoiding alcohol-related deaths post-transplant (Lee et al. 2018).
Metrics for determining successful liver transplantation should be an ongoing area of discussion in the field. There remains a need for comprehensive analyses of post-liver transplant outcomes in addition to calculating survival rates. Post-transplant outcomes such as recidivism, quality of life, financial and social stability, and more need to be analyzed to better understand how to treat and support individuals with ALD.
Consideration for non-expedited liver transplantation
When discussing early-liver transplantation for patients with acute AH, it is important to consider the potential inequalities of early-liver transplant approval for patients with ALD compared to patients with chronic liver diseases. Typically, acute AH patients are hospitalized and considered for liver transplantation during the peak of an alcohol binge, when liver injury is at its worst. Because of this, patients with acute AH typically present with high MELD scores and hence are expedited in prioritization on the liver transplant waitlist. The rationale is that people who acutely need new livers today will receive new livers first.
This can be viewed as problematic and possibly even unfair. It is argued that an inequitable system has been created where prioritization is granted to individuals with acute AH compared to patients who have chronic liver conditions that are slow-progressing and indicate with low MELD scores. In many cases, individuals with slow-progressing chronic liver diseases need liver transplantation to improve quality of life and survival, yet many of them will not receive an expedited transplant unlike individuals with acute AH.
It was suggested at the ALD Emerging Topics conference that a potential solution could be to slow down the speed of expedited early-liver transplantation approval of patients with acute AH. As stated above, individuals with acute AH usually receive medical attention while they are at the peak of an alcohol binge. It has been proposed that waiting a longer time period before granting liver transplantation will allow other patients with chronic liver diseases to receive liver transplants. Slowing down the accelerated rate of early-liver transplantation in acute AH cases may promote more equity with other chronic liver disease patients who are waiting to receive a new liver.
AUD Treatment
AUD is a serious condition that is described as the inability to stop or control alcohol use regardless of adverse effects on health, occupational, or psychosocial factors (NIAAA 2021). AUD cases are rising, yet only approximately 7% of AUD patients receive treatment (NIAAA 2022). AUD is considered a leading cause of preventable death (Yang et al. 2022). It is perhaps reflective of the current state of ALD care that the section discussing AUD comes at the end of this post. As revealed by the low rate of AUD treatment, there is a somewhat hindsight approach to AUD treatment. It can be argued that AUD treatment is not sought after or provided frequently enough at early stages in order to prevent the occurrence of liver injury and ALD.
AUD treatment can involve behavioral therapies, support groups, nutritional therapies, and medications (NIAAA 2021). Investments in mental health services, addiction services, education, and early intervention save long-term costs of treatments, transplants, and premature deaths. Integrated care from transplant centers and addiction specialists is a great strategy to support alcohol abstinence and complements ALD treatment. Ideally, integrated care would involve the co-location of all providers, laboratories, and treatments to the same site. Alcohol recidivism following liver transplantation is associated with negative outcomes, such as graft rejection and death (Arab et al. 2022). Thus, the optimization of AUD treatment pre- and post-liver transplantation should be further investigated to better support long-term abstinence and survival (Arab et al. 2022).
In actuality, there are many barriers to the successful integration of AUD and ALD care. There are attitudes and stigmas surrounding AUD that limit access to care. Logistical challenges, psychosocial concerns, and minimal or absent insurance coverage are each significant obstacles to overcome in order to fully integrate AUD and ALD care.
Conclusion
In summary, better biomarkers are needed to accurately diagnose AH, clearly stratify ALD/AH severity, and predict outcomes following steroid treatment. There is a need to accurately identify which patients need a liver transplant and which patients will improve on their own. Early liver transplantation offers hope to patients with acute AH, especially in cases where therapeutics are not effective. In order to provide integrated, holistic care, there is great work to be done to overcome the stigma surrounding alcohol use along with improving access to care. The ALD experts and addiction specialists in attendance at the ALD Emerging Topics Conference shed light on this important topic, thoroughly highlighting the need for more discussion and progress in order to better serve individuals with ALD.
Further Reading
Arab JP, Díaz LA, Baeza N, Idalsoaga F, et al. Identification of optimal therapeutic window for steroid use in severe alcohol-associated hepatitis: A worldwide study. J Hepatol. 2021 Nov;75(5):1026-1033. doi: 10.1016/j.jhep.2021.06.019. Epub 2021 Jun 21. PMID: 34166722.
Arab JP, Izzy M, Leggio L, Bataller R, Shah VH. Management of alcohol use disorder in patients with cirrhosis in the setting of liver transplantation. Nat Rev Gastroenterol Hepatol. 2022 Jan;19(1):45-59. doi: 10.1038/s41575-021-00527-0. Epub 2021 Nov 1. PMID: 34725498; PMCID: PMC8559139.
Cholankeril G, Ahmed A. Alcoholic Liver Disease Replaces Hepatitis C Virus Infection as the Leading Indication for Liver Transplantation in the United States. Clin Gastroenterol Hepatol. 2018 Aug;16(8):1356-1358. doi: 10.1016/j.cgh.2017.11.045. Epub 2017 Dec 1. PMID: 29199144; PMCID: PMC6467713.
HRSA, Scientific Registry of Transplant Recipients. OPTN/SRTR 2020 Annual Data Report: Liver. https://srtr.transplant.hrsa.gov/annual_reports/2020/Liver.aspx#:~:text=In%202020%2C%20despite%20 the%20COVID,425%20living%20donor%20liver%20transplants. Accessed 20 October 2022.
Kaplan A, Wahid N, Fortune BE, Verna E, Halazun K, Samstein B, Brown RS Jr, Rosenblatt R. Black patients and women have reduced access to liver transplantation for alcohol-associated liver disease. Liver Transpl. 2022 Jul 18. doi: 10.1002/lt.26544. Epub ahead of print. PMID: 35848134.
Kwon TJ, Kang W, Gwak GY, Paik YH, Choi MS, Lee JH, Koh KC, Sinn DH, Paik SW. Outcome of patients with severe alcoholic hepatitis after Model for End-Stage Liver Disease-based allocation system implementation in Korea. Korean J Transplant. 2021 Mar 31;35(1):24-32. doi: 10.4285/kjt.20.0054. PMID: 35769621; PMCID: PMC9235328.
Lee BP, Mehta N, Platt L, Gurakar A, Rice JP, Lucey MR, Im GY, Therapondos G, Han H, Victor DW, Fix OK, Dinges L, Dronamraju D, Hsu C, Voigt MD, Rinella ME, Maddur H, Eswaran S, Hause J, Foley D, Ghobrial RM, Dodge JL, Li Z, Terrault NA. Outcomes of Early Liver Transplantation for Patients With Severe Alcoholic Hepatitis. Gastroenterology. 2018 Aug;155(2):422-430.e1. doi: 10.1053/j.gastro.2018.04.009. Epub 2018 Apr 12. PMID: 29655837; PMCID: PMC6460480.
Lee BP, Vittinghoff E, Dodge JL, Cullaro G, Terrault NA. National Trends and Long-term Outcomes of Liver Transplant for Alcohol-Associated Liver Disease in the United States. JAMA Intern Med. 2019 Mar 1;179(3):340-348. doi: 10.1001/jamainternmed.2018.6536. Erratum in: JAMA Intern Med. 2019 Dec 1;179(12):1739. PMID: 30667468; PMCID: PMC6439700.
Matthews LA, Lucey MR. Psychosocial Evaluation in Liver Transplantation for Patients with Alcohol- Related Liver Disease. Clin Liver Dis (Hoboken). 2022 Jan 24;19(1):17-20. doi: 10.1002/cld.1160. PMID: 35106144; PMCID: PMC8785917.
McElroy LM, Likhitsup A, Scott Winder G, Saeed N, Hassan A, Sonnenday CJ, Fontana RJ, Mellinger J. Gender Disparities in Patients With Alcoholic Liver Disease Evaluated for Liver Transplantation. Transplantation. 2020 Feb;104(2):293-298. doi: 10.1097/TP.0000000000002843. PMID: 31283683; PMCID: PMC8173276.
Millson C, Considine A, Cramp ME, Holt A, Hubscher S, Hutchinson J, Jones K, Leithead J, Masson S, Menon K, Mirza D, Neuberger J, Prasad R, Pratt A, Prentice W, Shepherd L, Simpson K, Thorburn D, Westbrook R, Tripathi D. Adult liver transplantation: A UK clinical guideline – part 1: pre-operation. Frontline Gastroenterol. 2020 Feb 25;11(5):375-384. doi: 10.1136/flgastro-2019-101215. PMID: 32879721; PMCID: PMC7447286.
National Institutes on Alcohol Abuse and Alcoholism (NIAAA). Understanding Alcohol Use Disorder. April 2021. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/understanding-alcohol-use-disorder. Accessed on October 24, 2022.
National Institutes on Alcohol Abuse and Alcoholism (NIAAA). Alcohol facts and statistics. March 2022. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-facts-and-statistics. Accessed on October 24, 2022.
Obed A, Stern S, Jarrad A, Lorf T. Six month abstinence rule for liver transplantation in severe alcoholic liver disease patients. World J Gastroenterol. 2015 Apr 14;21(14):4423-6. doi: 10.3748/wjg.v21.i14.4423. PMID: 25892898; PMCID: PMC4394109.
Rice JP, Lucey MR. Should length of sobriety be a major determinant in liver transplant selection? Curr Opin Organ Transplant. 2013 Jun;18(3):259-64. doi: 10.1097/MOT.0b013e32835fb94b. PMID: 23492643.
Shield KD, Parry C, Rehm J. Chronic diseases and conditions related to alcohol use. Alcohol Res. 2013;35(2):155-73. PMID: 24881324; PMCID: PMC3908707.
Singal AK, Walia I, Singal A, Soloway RD. Corticosteroids and pentoxifylline for the treatment of alcoholic hepatitis: Current status. World J Hepatol. 2011 Aug 27;3(8):205-10. doi: 10.4254/wjh.v3.i8.205. PMID: 21954408; PMCID: PMC3180605.
Tang KY, Lickliter J, Huang ZH, Xian ZS, Chen HY, Huang C, Xiao C, Wang YP, Tan Y, Xu LF, Huang YL, Yan XQ. Safety, pharmacokinetics, and biomarkers of F-652, a recombinant human interleukin-22 dimer, in healthy subjects. Cell Mol Immunol. 2019 May;16(5):473-482. doi: 10.1038/s41423-018-0029-8. Epub 2018 Apr 18. PMID: 29670279; PMCID: PMC6474205.
Tapper EB, Parikh ND. Mortality due to cirrhosis and liver cancer in the United States, 1999-2016: observational study. BMJ. 2018 Jul 18;362:k2817. doi: 10.1136/bmj.k2817. PMID: 30021785; PMCID: PMC6050518.
Volk ML, Biggins SW, Huang MA, Argo CK, Fontana RJ, Anspach RR. Decision making in liver transplant selection committees: a multicenter study. Ann Intern Med. 2011 Oct 18;155(8):503-8. doi: 10.7326/0003-4819-155-8-201110180-00006. PMID: 22007044; PMCID: PMC3197782.
WHO. Alcohol: Fact sheet. 9 May 2022. https://www.who.int/en/news-room/fact-sheets/detail/alcohol. Accessed 19 October 2022.
Yang W, Singla R, Maheshwari O, Fontaine CJ, Gil-Mohapel J. Alcohol Use Disorder: Neurobiology and Therapeutics. Biomedicines. 2022 May 21;10(5):1192. doi: 10.3390/biomedicines10051192. PMID: 35625928; PMCID: PMC9139063.
ML-00-01003Rev01