In vitro Liver Culture Systems to Investigate DILI
Posted on: July 8, 2021
In vitro Liver Culture Systems to Investigate DILI
Contributed by Abi Kasberg, PhD
An important function of the liver is to concentrate and metabolize drugs and xenobiotics, which makes the liver vulnerable to tissue damage. Drug-induced Liver Injury (DILI) is the onset of liver damage caused by drugs, medications, or supplements. DILI is associated with hepatotoxicity, acute liver failure, and chronic liver disease. The most common medications known to cause DILI are antibiotics, anesthetics, anticancer drugs, antiretrovirals, cardiac drugs, and acetaminophen, although liver injury can be caused by nearly every class of medication. DILI is commonly detected and monitored by serum biomarkers. The most effective way to treat DILI is to immediately discontinue use of the DILI-causing substance. Therefore, DILI is frequently the reason for withdrawal of preclinical and clinical drugs from the healthcare market.
To prevent late withdrawal of drugs and failure of clinical studies, there is a need for in vitro liver models that reflect human livers to screen for hepatotoxicity and DILI potential during early drug development. Animal model systems fall short of providing an accurate replication of the complex human liver system during preclinical toxicity studies. Several in vitro human liver culture systems have been developed for the prediction of DILI and hepatotoxicity including 2D monolayer cell culture, 3D liver models, liver-chip technology, micropatterned co-culture (MPCC), 3D liver bioprinting, and hollow fiber bioreactors. These liver culture systems are used to evaluate liver function and screen preclinical drug candidates for the purpose of assessing liver safety through the examination of DILI biomarkers.
Phases of drug metabolism in the liver
During drug metabolism, drugs are broken down and metabolized into less toxic, hydrophilic compounds that can be excreted from the body. The rate of drug metabolism dictates the duration and impact of drug functionality. As drugs are metabolized, it is important to consider that drug intermediates can also have toxic effects on the body.
The goal of drug metabolism is to biotransform chemical compounds into water-soluble components that can be easily eliminated from the body. Biotransformation largely occurs in the liver through 3 enzymatic processes termed phase I, phase II, and phase III (Fig 1). Phase I requires functionalization enzymes, such as cytochrome P450 enzymes, to introduce and transfer functional groups onto the drug compound. Phase II enzymes, including N-acetyltransferases, conjugate the modified chemical compounds with polar compounds that are necessary for excretion. When the conjugated chemical compound requires further processing, phase III transporters facilitate elimination via efflux mediators. Phase III transporters are expressed in the liver and include ATP binding cassette (ABC) transporters, which function to facilitate the movement, or efflux, of water soluble and polarized compounds across phospholipid membranes and out of cells. When reviewing in vitro liver models, it is important to evaluate the activity of drug metabolizing enzymes and transporters (DMETs) in the liver culture system for the most accurate assessment of DILI potential.
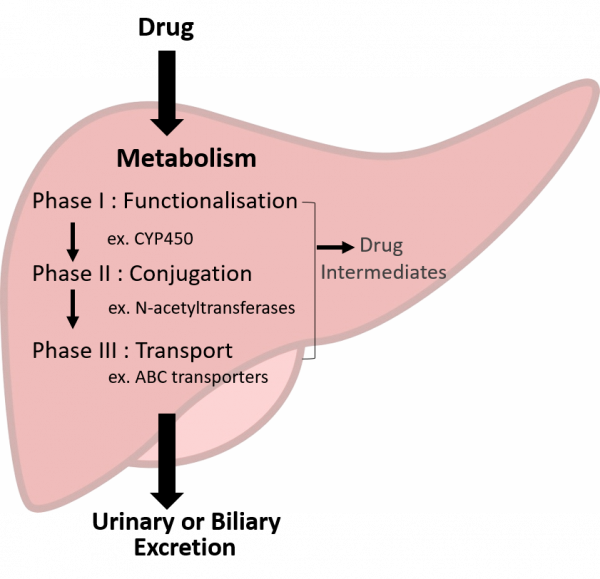
Figure 1: Drug metabolism in the liver occurs in three phases (I-III) to facilitate excretion of the metabolized compound out of the body.
In vitro human liver culture systems
Two important features to consider when utilizing in vitro liver models are 1) the conservation of liver function, such as albumin secretion, and 2) adequate expression of phase I, II, and III DMETs (Zhou et al 2019). These two attributes will best equip in vitro liver models to be reliable and consistent predictors of DILI and hepatotoxicity.
In 2D monolayer culture, cells are cultured on a flat surface resulting in a single layer of cells that have flat and stretched morphologies (Fig 2)(Edmondson et al 2014). Due to simplicity in assay setup and cost-effectiveness, 2D monolayer culture is a popular in vitro liver model for assessing hepatotoxicity and drug metabolism (Gupta et al. 2021). A variety of liver cell lines are commonly used for 2D monolayer cell culture:
- Primary human hepatocyte (PHH) culture is considered the gold standard of liver cell culture systems. PHH maintains the expression of phase I and phase II enzymes, as well as phase III transporters, but only for a brief time in culture (Kuna et al 2018, Zhou et al 2019). Over time, PHHs experience rapid dedifferentiation in monolayer culture which contributes to declining levels of metabolizing enzymes (Zhou et al 2019).
- Differentiation of human pluripotent stem cell lines (hPSCs) and human induced pluripotent stem cells (hiPSCs) into hepatic cells have shown potential for studying liver toxicity. In fact, hPSCs appear to be more accurate in analyzing toxicity than hepatocarcinoma-derived cell lines (Kuna et al 2018).
- Cell lines derived from hepatoma cells have abundant propagation potential, but most hepatoma cell lines, such as HepG2, do not contain adequate levels of metabolizing enzymes and typically lack adequate hepatocyte functionality (Kuna et al 2018). On the other hand, liver tumor HepaRG cells show nearly comparable levels of phase I and phase II enzymes compared to human liver samples. HepaRG cells are widely used to evaluate drug-induced hepatotoxicity and have shown to be sufficient in analyzing drug toxicity of some but not all drug agents in vitro (Kuna et al 2018).
- In addition to these, other cell lines are being used to evaluate liver drug metabolism such as recombinant cells expressing cytochrome P450 and hepatic cell lines transfected with vectors expressing drug metabolizing enzymes (Kuna et al 2018).
It is important to keep in mind that the unusual cellular morphologies associated with 2D monolayer culture impacts cellular processes including proliferation, apoptosis, and cell signaling. Drugs commonly target specific cell surface receptors, which makes cell morphology and spatial arrangement within the culture environment to be key factors while discerning drug toxicities (Edmondson et al 2014). As such, 2D monolayer cultures have heightened cellular responses and efficacies to drug exposure, which are not reflective of in vivo or 3D liver culture drug responses.
2D Monolayer Cell Culture
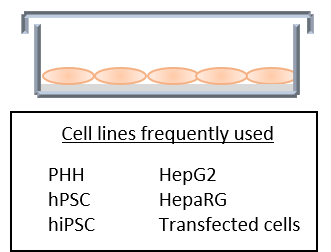
Figure 2: 2D monolayer cell culture results in the growth of a single layer of flat cells. A variety of cell types can be used for in vitro liver culture systems including primary human hepatocytes (PHH), human pluripotent stem cells (hPSC), human induced pluripotent stem cells (hiPSC), hepatoma cell lines HepG2 and HepaRG, along with cells transfected with vectors expressing metabolizing enzymes.
3D liver cultures have been developed to overcome shortcomings associated with 2D monolayer cell culture models. Culturing cells in 3D more accurately reflects in vivo cellular responses that are dependent on cell morphology and spatial organization, such as cell surface receptors. The added dimensionality of 3D cultures improves hepatocyte functionality and DMET expression, along with a more sensitive and accurate capacity to detect hepatotoxicity compared to 2D monolayer cell culture (Cox et al 2020). 3D liver culture systems are typically composed of liver spheroids or liver organoids. Liver spheroids are cells that aggregate to form a spherical structure. Spheroids may contain more than one cell type and can perform a function specific to the liver (Cox et al 2020). Liver organoids are self-organizing 3D structures that contain multiple cell types and function in capacities specific to the liver. Organoids develop in response to cell-to-cell interactions and developmental cues (Cox et al 2020). Multicellular 3D cultures are suggested to have more biological significance and are better equipped to react to drug toxicities due to the involvement of multiple cell types (Cox et al 2020). Liver organoids and liver spheroids can either self-aggregate in scaffold-free systems or they can be cultured in a scaffold-based platforms.
Scaffold-Free vs. Scaffold-based TechniquesScaffold-free culture systems utilize the cellular ability of cells to self-aggregate in the absence of cell attachment substrates (Zhou et al 2019). 3D scaffold-free spheroids or organoids are commonly formed via hanging drop suspension, rotating bioreactors, or in multi-well plates with ultra-low cell attachment surfaces (Fig 3). Scaffold-based culture methods are used to provide stability, size consistency, and assistance to 3D organotypic liver cultures. Biological scaffolds function to facilitate the accumulation of important elements of the hepatic microenvironment, such as collagens and fibronectin, that are necessary for hepatic tissue organization, cell signaling, and cell fate (Cox et al 2020, Selden et al., 2000, Zhou et al 2019). Scaffolds are commonly composed of polysaccharides, alginate, collagen, or nanofibrous poly-L-lactic acid to best support liver spheroid development. Scaffolds provide a physical platform for the culture of specific cellular arrangements, as seen with bioprinting techniques (Fig 3, see section on “3D liver bioprinting” below). During scaffold-based 3D culture studies, it is important to consider the potential influence that scaffolds may have on drug diffusion and binding, toxicity, and batch variability of scaffolding materials (Cox et al 2020, Zhou et al 2019). |
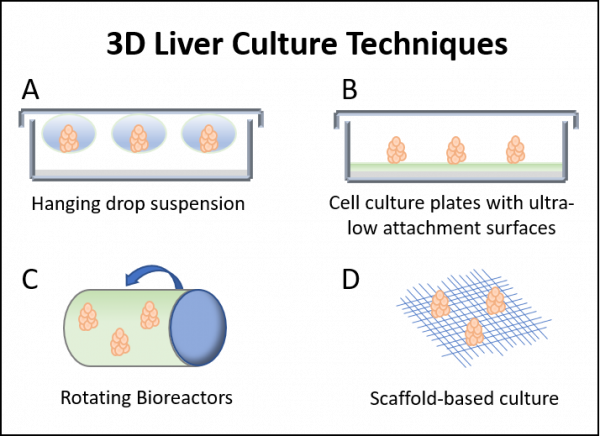
Figure 3: 3D liver culture techniques include (A) hanging drop suspension, (B) cell culture plates coated with ultra-low cell attachment surfaces, (C) rotating bioreactors, and (D) scaffold-based culture systems.
3D liver spheroid models are high quality, in vitro options for assessing DILI due to preserved tissue architecture that closely resembles the cellular organization of the in vivo liver. 3D liver spheroids show improved hepatic cell function and expression of metabolizing enzymes compared to monolayer cell culture (Zhou et al 2019). 3D liver spheroids portray increased hepatotoxicity after extended exposure to toxic compounds suggesting that 3D liver models are suitable for analyzing chronic DILI (Bell et al 2016, Kuna et al 2018). Liver spheroids can be developed from PHH, hiPSC, or hepatic cell lines HepG2 and HepaRG:
- PHH-derived spheroids have a longer viability timeline compared to PHH monolayer culture and can be co-cultured with non parenchymal cells (NPCs) that are important for the liver microenvironment (Zhou et al 2019). In a comparative proteome analysis, PHH spheroids expressed proteomic data similar to the proteome of donor hepatic tissue, suggesting that the enzymatic activity of DMETs is preserved in PHH spheroids (Kuna et al 2018, Schyschka et al 2013, Zhou et al 2019). PHH spheroids can also replicate liver diseases, including steatosis and cholestasis, which introduces the opportunity for studying DILI during pathological states (Lin et al 2016).
- Spheroids generated using hepatocyte-like cells obtained from hiPSCs are appealing because they can be generated in a patient-specific manner. This creates a powerful opportunity to investigate patient-specific drug toxicities and reactions (Zhou et al 2019). At this point in time, hiPSC differentiation protocols are still being developed in the 3D liver spheroid culture system and hepatotoxicity data is limited. More research in this area is needed.
- HepG2 spheroid cultures show improved phase III transporter expression and enhanced liver functionality compared to HepG2 monolayer culture. HepG2 spheroids are well suited for high-throughput screening studies and are capable of predicting hepatotoxicity of acetaminophen, amiodarone, diclofenac, metformin, phenformin, paracetamol, and valproic acid (Fey et al 2020, Zhou et al 2019). HepaRG spheroids show greater metabolic enzyme activity and are likewise more sensitive to toxicity for some but not all drug compounds when compared to HepaRG monolayer culture (Zhou et al 2019).
To accompany these advantages, it is important to keep in mind that 3D spheroid liver models are missing various vascular cell types and do not fully reproduce immune-mediated responses, which contribute to hepatotoxicity (Kuna et al 2018). Despite 3D spheroid models not being exact reproductions of in vivo livers, they do provide powerful preclinical tools for the prediction of DILI and liver damage.
3D liver organoids can be derived from pluripotent stem cells, liver progenitor cells, fetal hepatocytes, or liver biopsy tissue. Organoids are developed through the careful management of signaling pathways while in culture. For example, liver progenitor cells can be isolated, expanded, and cultured with exogenous developmental growth factors, such as EGF, FGF, Wnt, Rspo, and TGF- β, to induce organogenesis (Fig 4) (Cox et al 2020). Once activated, these bipotent liver progenitor cells undergo incredible self-organization to form functional organoids (Cox et al 2020). Hepatic organoids contain epithelial compartments that are similar to in vivo hepatic ductal compartments. They also have high expression levels of hepatocyte markers and increased liver functionality (Cox et al 2020 ). Patient-specific liver models can be generated from adult stem cells or hiPSCs. Organoids that contain hepatobiliary structures have been successfully generated from hiPSCs and human fetal liver progenitor cells (Vyas et al 2018, Wu et al 2019). Hepatic organoids retain DMET expression levels, making them attractive in vitro models for assessing DILI and liver function. However, there are concerns surrounding consistency of organoid culture conditions, production efficiency, and reproducibility (Cox et al 2020).
3D Liver Organoids

Figure 4: 3D liver organoids are derived from liver progenitor cells that are isolated and expanded in culture. After the addition of growth factors, such as EGF, FGF, Wnts, Rspo, and TGF-β, activated liver progenitor cells undergo organogenesis to form complex and functional liver organoid tissues.
3D liver bioprinting is a method that deposits cells in a highly specific spatial and temporal manner. For instance, bioprinting techniques can strategically place liver stromal cells in specific proximity to hepatocytes, which can promote liver compartmentalization and microvascular development (Lin et al 2016). Two common methods of bioprinting include droplet-based bioprinting and extrusionbased bioprinting (Fig 5):
- Droplet-based bioprinting (DBB) uses droplets to produce heterocellular 3D culture systems. For example, DBB can create a heterogeneous mix of HepG2 and HUVEC cell lines in a model that is capable of albumin secretion and cytochrome P450 enzymatic activity (Zhou et al 2019).
- Unlike droplet deposition techniques, extrusion-based bioprinting (EBB) deposits continuous strands of cells in a highly versatile method that is compatible with 3D spheroid cultures. 3D structures of liver HepG2 cells that express hepatic biomarkers have been created using EBB (Jeon et al 2017).
3D bioprinting requires bioink, which is composed of cells of interest that are encapsulated in extracellular material. Hepatotoxicity and DILI studies have successfully been performed using bioprinted livers, including a liver-chip model (Knowlton and Tasoglu 2016, Nguyen et al 2016, Zhou et al 2019). 3D liver bioprinting is a promising and innovative technology for use in drug metabolism and DILI analyses.
3D Liver Bioprinting
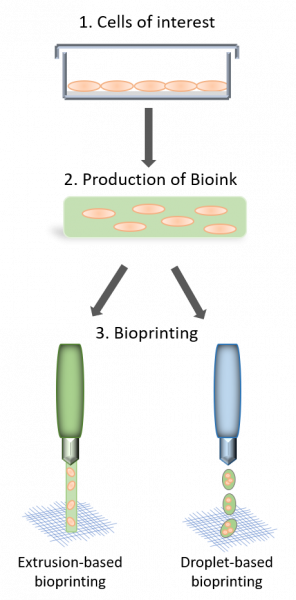
Figure 5: 3D Bioprinting methods utilize bioink to place a heterogenous mix of cells in a spatially-specific manner. Two common bioprinting methods used to generate 3D livers are extrusion-based bioprinting and droplet-based bioprinting.
Liver-chip technology has recently made remarkable advances in replicating organ-level functionality for drug screening purposes. Liver-chips are microfluidic devices that cultivate species specific 3D liver microenvironments in adept in vitro culture systems. Liver-chips incorporate a variety of critical cell types, such as hepatocytes, endothelial cells, stellate cells, and Kupffer cells in culture under physiological fluid flow conditions (Fig 6). Media-perfused environments mimic liver vascularization and contribute to 3D liver architecture (Kuna et al 2018, Zhou et al 2019). Specific liver function can be generated with hiPSCs or PHH liver cells (Kuna et al 2018). Liver function and DMET expression are largely maintained in liver-chip models. DILI research studies using liver-chips have successfully detected liver toxicity via measurement of DILI biomarkers (Jang et al 2019). Together, this makes the liver-chip culture system a clever and excellent in vitro model to use for hepatotoxicity and DILI studies.
Liver-Chip
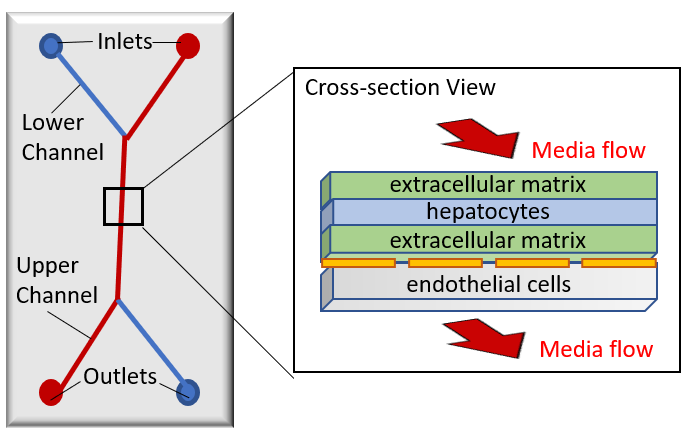
Figure 6: Liver-chips culture a variety of cell types to replicate a liver system. Note that liver-chips vary in design and composition. Liver-chips are typically composed of two channels, an upper channel depicted in red and a lower channel in blue. Channels are separated by a porous membrane (dotted orange line). Cells of interest, such as hepatocytes, endothelial cells, and Kupffer cells, can be cultured in either the upper or lower channel to create 3D architecture. In perfused liver-chip models, media flows directionally from inlets to outlets.
Micropatterned co-culture (MPCC) is a microliver platform in which hepatic PHH or hiPSC cells are seeded on islands of extracellular matrix substrate and surrounded by stromal cells (Fig 7) (Lin et al 2016, Zhou et al 2019). This system enables specific control over hepatocyte microenvironments, cellular interactions, and cellular architecture to promote dependable liver function (Lin et al 2016). While investigating DILI, MPCCs can be enhanced with liver sinusoidal endothelial cells and hepatic stellate cells to encourage liver cell crosstalk (Lin et al 2016). MPCCs retain drug metabolism characteristics, phase III transporters, and show high similarity to the human liver (Zhou et al 2019). MPCCs are widely used during many phases of drug development due to high specificity and moderate sensitivity during hepatotoxicity studies (Khetani et al 2013).
Micropatterned Co-culture
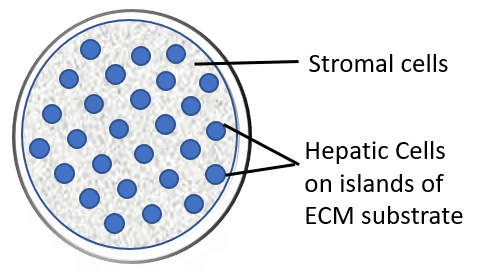
Figure 7: Micropatterned co-culture (MPCC) systems use islands of extracellular matrix (ECM), such as collagen, to culture PHH or hiPSC-derived liver cells. The ECM islands are surrounded by stromal cells that are needed during drug metabolism and liver function.
Hollow fiber bioreactors provide an additional in vitro perfusion-based method for developing semivascularized organotypic hepatocyte cultures. There are many benefits of perfusion-based models; the vascularity of the organ is recapitulated, shear forces are included, flow conditions allow cell types to be interconnected through the transport of signaling molecules, and concentration gradients of nutrients, molecules, and gasses can be replicated (Cox et al 2020). The hollow fiber bioreactor culture setup is composed of capillaries that permeate tubular modules (Fig 8). Hepatic cells are cultured in the extra-capillary space of these tubes. Capillaries supply hepatic cells with oxygen and nutrient-rich medium via perfusion (Ebrahimkhani et al 2015). This liver culture setup uniquely imitates capillary blood-tissue fluid exchange in a semi-vascularized liver model that protects cells from shear stress (Ebrahimkhani et al 2015, Zhou et al 2019). This makes the hollow fiber bioreactor model a superb choice for long-term hepatic function and maintenance studies. Hepatic function, metabolic enzymatic activity, and transporter activity is preserved in this model using PHH or HepaRG cells, although PHHs appear to perform better than HepaRGs (Zhou et al 2019). A drawback to hollow fiber bioreactors is that they require a large quantity of cells which makes them inefficient for use in high-throughput hepatotoxicity studies. Structural components of the bioreactor system may also interfere with drug absorption, which could make drug toxicity studies problematic (Zhou et al 2019).
Hollow Fiber Bioreactor
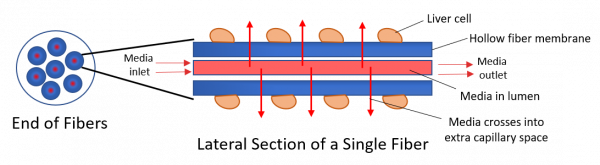
Figure 8: Hollow fiber bioreactors facilitate the perfusion of media through a hollow lumen. The media crosses the fiber membrane to supply the liver cells located in the extra-capillary space with nutrients
(Figure adapted from Zhou et al 2019).
Human liver culture summary
Hepatotoxicity and DILI studies most commonly use 2D monolayer cultures, 3D liver models, MPCC, and liver-chip in vitro models. Acetaminophen exposure is frequently used during the evaluation of model sensitivity and hepatotoxicity. Liver spheroids developed from PHHs are suggested to be the most sensitive model for detecting acetaminophen toxicity in vitro (Zhou et al 2019). Liver-chip technology is extremely promising for predicting DILI, and MPCC systems are particularly valuable when utilizing hiPSC-derived hepatic cells for liver function studies (Zhou et al 2019). Altogether, more research studies are needed that compare in vitro liver models to human livers. This will help to determine relevance of each in vitro liver model and their ability to accurately predict DILI and hepatotoxicity.
DILI biomarkers for use in human liver culture models
DILI is commonly detected through serum biomarkers. Monitoring serum DILI biomarker levels enables liver injury to be measured and recorded during drug development and administration. Traditional liver biomarkers, such as alanine aminotransferase (ALT) and aspartate aminotransferase (AST), lack specificity to liver injury and fail to sensitively predict DILI potential (Church et al 2017).
As an alternative to standard DILI biomarkers, caspase cleaved cytokeratin 18 (cck18) and total keratin 18 (K18) serum or supernatant levels can be measured as sensitive, specific, and predictive DILI biomarkers. ccK18 functions as a highly specific biomarker of hepatocyte apoptosis and K18 is a biomarker for total hepatocyte cell death. When used together, mechanistic information on liver cell death can be learned and leveraged for the evaluation of drug safety. Additional emerging biomarkers being studied to predict DILI include osteopontin (OPN) to detect hepatic inflammation and necrosis, alpha glutathione S-transferase (aGST) which is sensitive to swift changes in hepatic injury and hepatotoxicity, and liver fatty acid binding protein (L-FABP) to detect hepatocyte leakage and damage.
Further Reading
Bell, CC., Hendriks, DFG., Moro, SML., et al. Characterization of primary human hepatocyte spheroids as a model system for drug-induced liver injury, liver function and disease. Sci Rep. 2016. May 4;6:25187. doi: 10.1038/srep25187.
Church, RJ. and Watkins, PB. The transformation in biomarker detection and management of drug induced liver injury. Liver Int. 2017 November ; 37(11): 1582–1590. doi:10.1111/liv.13441.
Cox, CR., Lynch, S., Goldring, C., and Sharma, P. Current Perspective: 3D Spheroid Models Utilizing Human-Based Cells for Investigating Metabolism-Dependent Drug-Induced Liver Injury. Front. Med. Technol. 2020. 30 November.
Ebrahimkhani, MR., Neiman, JAS., et al. Bioreactor Technologies to Support Liver Function In Vitro. Adv Drug Deliv Rev. 2014. April. 132–157. doi:10.1016/j.addr.2014.02.011.
Edmondson, R., Broglie, JJ., Adcock, AF., and Yang, L. Three-Dimensional Cell Culture Systems and Their Applications in Drug Discovery and Cell-Based Biosensors. Assay Drug Dev Technol. 2014. May 1; 12(4): 207–218. doi: 10.1089/adt.2014.573
Fey, SJ. Korzeniowska, B., and Wrzesinski, K. Response to and recovery from treatment in human liver-mimetic clinostat spheroids: a model for assessing repeated-dose drug toxicity. Toxicology Research. 2020, 9, 379–389.
Gupta, R., Schrooders, Y., Hauser, D., et al. Comparing in vitro human liver models to in vivo human liver using RNA‑Seq. Archives of Toxicology. (2021) 95:573–589.
Jeon, H., Kang, K., Park, SA., et al. Generation of multilayered 3D structures of HepG2 cells using a bioprinting technique. Gut and Liver. 2017. 11, 121–128.
Khetani, S. R., Kanchagar, C., Ukairo, O., et al. Use of micropatterned cocultures to detect compounds that cause drug-induced liver injury in humans. Toxicol. Sci. 2013. 132, 107–117.
Knowlton, S. and Tasoglu, S. A bioprinted liver-on-a-chip for drug screening applications. Trends Biotechnol. 2016. 34, 681–682.
Kuna, L., Bozic, I., Kizivat, T., et al. Models of Drug Induced Liver Injury (DILI) – Current Issues and Future Perspectives. Current Drug Metabolism. 2018, 19, 830-838.
Nguyen, DG., Funk, J., Robbins, JB., et al. Bioprinted 3D primary liver tissues allow assessment of organ-level response to clinical drug induced toxicity in vitro. PLoS One. 2016. 11, e0158674–17.
Schyschka, L., Sanchez, JJM., Wang, Z., et al. Hepatic 3D cultures but not 2D cultures preserve specific transporter activity for acetaminophen-induced hepatotoxicity. Arch Toxicol. 2013. Aug;87(8):1581-93.
Selden, C., Khalil, M., and Hodgson, H. Three dimensional culture upregulates extracellular matrix protein expression in human liver cell lines—a step towards mimicking the liver in vivo? Int. J. Artif. 2000. Organs 23, 774–781.
Vyas, D., Baptista, PM., Brovold, M., et al . Self-assembled liver organoids recapitulate hepatobiliary organogenesis in vitro. Hepatology. 2018;67:750–61.
Wu, F., Wu, D., Ren, Y., et al . Generation of hepatobiliary organoids from human induced pluripotent stem cells. J Hepatol. 2019. 70:1145–58.
Zhou, Y., Shen, JX., and Lauschke, VM. Comprehensive Evaluation of Organotypic and Microphysiological Liver Models for Prediction of Drug-Induced Liver Injury. Frontiers in Pharmacology. 2019. Sep 24;10:1093. doi: 10.3389/fphar.2019.01093.
ML-00-00830 Rev01