Anticipated NASH Drug Approval will Require Expanded Non-Invasive Testing: NASH-TAG 2023 Takeaways
Posted on: April 19, 2023
-Contributed by Abi Kasberg, PhD
High levels of enthusiasm and excitement were shared at this year’s NASH-TAG meeting in Deer Valley, Utah, regarding the future of the NASH landscape. This was in large part due to the announcement of positive data from two phase 3 clinical trials for new NASH drugs: Madrigal’s Resmetirom and Intercept’s Obeticholic Acid. Stimulating further excitement, Novo Nordisk’s approved obesity drug, Semaglutide, is also in trials for a new indication to treat NASH. These revelations became a beacon of hope that one or more NASH drugs are on track to be approved by regulators as soon as this year. If and when the anticipated regulatory approval occurs, this would mark the first time in the United States’ regulatory history that a therapeutic would be approved and available for the treatment of NASH. History in the making!
Furthermore, these positive readouts are monumental for the NASH space because they show that clinical trial endpoints are achievable in NASH phase 3 clinical trials. As it currently stands, NASH clinical trial endpoints are dependent on histologic scoring systems, which are problematic and considered to be a significant hinderance to the approval of new NASH drugs. However, these positive readouts show that the histologic endpoints can actually be met in NASH clinical trials.
In addition to spreading a message of optimism and excitement for approved NASH therapeutics, another key widespread discussion of the meeting was the importance and urgency to invest in non-invasive testing options for NASH. The need for non-invasive tests (NITs) are two-fold: NITs are needed to accompany new and ongoing clinical trials as readouts on outcome. NITs are also going to be needed clinically, to monitor response to treatment, likely in the near future. Hence, continued work to prepare NITs for these important applications is needed now.
Together, these latest phase 3 findings and key discussions are stimulating an increase of energy and enthusiasm that was tangible at the NASH-TAG 2023 meeting. NASH work is accelerating, and efforts are being prioritized to engage with the forward moving momentum of the NASH space.
Non-Invasive Testing Roles are Expanding
During the anticipated and historical next phase of NASH work, attention must be attuned to the advancement and application of NITs. Beautiful groundwork has been sown into developing a diverse menu of non-invasive testing options. The Madrigal and Intercept studies have demonstrated how to leverage NITs for clinical trial purposes. Now that we are approaching the starting line for a great transformation in NASH care, we will begin to see NITs fill roles in two separate capacities (Fig. 1). First, NITs will continue to support clinical trials with expanded roles. Following regulatory approval of new NASH therapeutics, NITs will move into novel capacities to support patient clinical care.
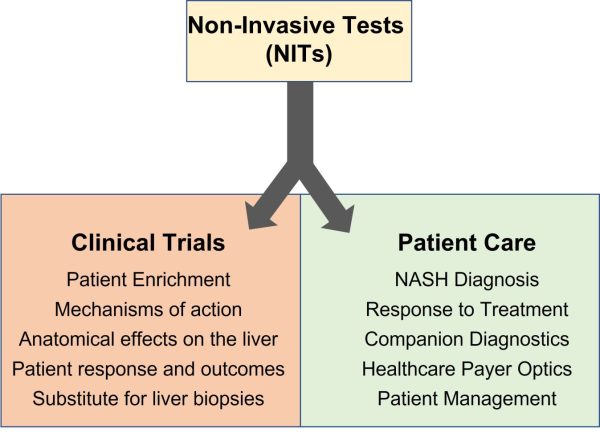
Figure 1: Non-invasive tests (NITs) will have dual utility as the future of the NASH landscape progresses. NITs will play important roles during clinical trials for new NASH drugs as well as providing important assistance during patient care.
Clinical Trials
Patient Enrichment
Careful patient population enrichment is the process of qualifying and selecting patients that will have the best opportunities to respond to the drug being tested. Enriched patient populations provide the greatest chances to generate supportive data demonstrating drug efficacy. Because trial enrichment is an important step in clinical trial design that could make or break a study, non-invasive testing readouts are powerful tools in selecting patient populations.
Mechanisms of Action and Effects on the Liver
Non-invasive testing menus that offer a wide breadth of knowledge can be used to further assess where in the anatomical liver the drugs are working, at what sensitivities, and which mechanisms of actions are being used.
Patient Response and Outcomes
NASH clinical trials endpoints require proof of histological benefit. This is problematic because paired liver biopsies followed by histologic analysis does not always correlate with patient responsiveness to a drug or outcome. Therefore, the NASH field needs biomarkers that are linked to outcomes and NITs that correlate with patient responsiveness. To help with this, NASH consortia including NIMBLE, LITMUS, GOLDMINE, NAIL-NIT have been organized to systematically assess the ability of NITs to correlate with endpoints.
Liver Biopsy Substitute
In addition to adding to the breadth of knowledge surrounding NITs and their mechanisms of actions, the eventual goal of these consortia is to identify NITs that could function as substitutes for paired liver biopsies. A coordinated effort is needed to change the regulatory requirements that are creating a bottleneck in NASH drug approvals in order to drive the agenda forward. At NASH-TAG 2023 there was an overall consensus to support the substitution of histological endpoints with non-invasive testing data that correlates with improved outcomes.
Patient Care
NASH Diagnosis
The future of non-invasive testing options in the clinical NASH environment will involve different purposes such as diagnosis, prognosis, and treatment response. Following the anticipated regulatory approval of new NASH drugs, AASLD guidelines will need to be updated regarding NASH diagnosis. This will likely include guidance on non-invasive testing readouts and the flow of sequential NITs to guide NASH treatment. NITs are changing liver portfolios not only in hepatology practices, but also in endocrinology and primary care. The American Diabetes Association is now recommending that NAFLD be screened for in patients with type II diabetes mellitus (Barbosa and Lai 2020). To do so, measurable indicators of outcomes, performance, and standards of care will be required. NIT optimization will provide relevance to guidelines, implementation, and clinical utility.
Response to Treatment
Critical aspects of patient-centered care involve careful monitoring of disease progression and assessing individual response to treatment. Following NASH drug approval, NITs will be leaned upon to refine drug monitoring protocols and to identify responders and non-responders to treatment. This is significant because 74%-76% of patients in the Madrigal Resmetirom trial were non-responders based on the histological criteria. Therefore, the ability to quickly identify who is responding to treatment and who is not, will provide a superior standard of patient-centric, individualized care.
Companion Diagnostics
There is a big need to identify response to drugs to prevent unnecessary costs and side effects. Along this line of thinking, it is ideal that companion diagnostics be developed as readouts for new drugs. Companion biomarkers can guide physicians and patients in treatment decisions. For NITs to be leveraged as companion diagnostics, continued effort is needed to standardize and optimize biomarkers.
Healthcare Payer Optics
Another perspective of patient care that must be considered is that of healthcare payers. Payers want optics on why the drug matters, who the drug is helping, and what is the expected progression. The ability to accurately identify response to treatment will work towards appeasing payers, so that only those we are receiving benefit from the drug will be treated with the drug. Definitions of therapeutic success, which is currently indicated as a regression of fibrosis, may need to be changed or refined. If 25% of patients achieve “success” while being treated with a new NASH drug, payers may not be willing to approve the cost when the response rate is low. However, if the definition of success is changed to be a readout on improved outcome, as indicated by NITs or biomarkers, the rate of reward could increase and hence provide greater satisfaction to payers.
Patient Management
In lieu of liver biopsies, the future of NASH involves the utility of NITs to assess and manage liver patients. NITs will function as tools to refine the management pathways in patient care. When used jointly or sequentially, NITs will assist with narrowing the indeterminate zone of patients who do not definitively test positive or negative for a NASH diagnosis. Algorithms and other easy-to-use tools that require minimal provider inputs are needed in order to accurately inform and manage patient care at the level of front-line and primary care. The encouraging news is that non-invasive testing options are already available that are diverse in terms of classification, specificity, sensitivity, and treatment response. In other words, the NITs that we have access to today are sufficient for use in patient care, given some additional efforts into standardization, optimization, and linking to outcomes.
Conclusions
The buzz in the air at NASH-TAG was filled with optimism and hope in anticipation of accelerated NASH drug approvals and the availability of diverse and informative non-invasive testing options. The NASH momentum is swiftly accelerating forward, and the outlook is looking bright.
Further Reading
Vieira Barbosa, Joana, and Michelle Lai. “Nonalcoholic Fatty Liver Disease Screening in Type 2 Diabetes Mellitus Patients in the Primary Care Setting.” Hepatology communications vol. 5,2 158-167. 31 Oct. 2020, doi:10.1002/hep4.1618
ML-00-01036 Rev01