Alcohol-related Clinical Trials & Early Liver Injury Biomarkers
Posted on: October 29, 2025
Contributed by Abigail Kasberg, PhD
Alcohol-related clinical trials play a fundamental role in advancing our understanding of the complex impact of alcohol consumption on human health. The prevalence of alcohol use is widespread, causing a systemic impact on the individual and affecting whole communities. Clinical trials are a means to investigate the mechanisms of alcohol-related diseases and evaluate the safety and efficacy of treatment interventions. Furthermore, clinical trials drive the discovery and utilization of relevant biomarkers to detect disease status within the body and mind. The ultimate goal of clinical studies is to create robust and safe evidence-based healthcare practices in order to best serve those with alcohol-related diseases.
For these reasons, the indications of alcohol use disorder (AUD), alcohol-associated liver diseases (ALD), and alcohol-associated hepatitis (AH) are currently being targeted for the development of new interventions and treatments. Biomarkers of early organ-specific damage and mechanistic probes into what initiates and drives disease pathology can be used to stratify subject populations, indicate response to treatment, and be motivators for behavioral therapies. In the context of alcohol-related clinical trials, reliable, valid, and accessible biomarkers of disease status and health outcomes need to be established to push the field of alcohol-related research forward. Here we provide a discussion surrounding the application of cytokeratin-18 (K18) M30® and M65® liver biomarkers during AUD, ALD, and AH clinical trials.
Alcohol-Use Disorder (AUD)
AUD is a brain disorder that is classically described as an inability to stop alcohol use. AUD can result in neurological changes to the brain that perpetuate AUD. The act of consuming alcohol will lead to neurological alterations that make it increasingly more difficult to stop consuming alcohol. AUD is described as a spectrum disease that is classified based on the number of symptoms the individual has. AUD is treated with behavioral therapies, support groups, and approved medications.
Alcohol-associated Liver Diseases (ALD)
ALD is a liver disease described as the onset of liver injury caused by heavy alcohol consumption. ALD is a spectrum disease ranging from mild steatosis, to steatohepatitis, to severe fibrosis and cirrhosis. ALD is treated with abstinence and in some cases, liver transplantation.
Acute Alcohol-associated Hepatitis (AH)
AH is a liver disease that is characterized by severe liver inflammation that is directly caused by alcohol consumption. AH symptoms include severe malnutrition and hepatic encephalopathy. AH diagnosis requires a liver biopsy. AH can be treated with prednisolone to improve 30-day mortality as well as liver transplantation. The use of prednisolone must be weighed against side effects and risks of treatment, such as increased risk of infection. Despite being a potentially life-saving option for individuals with AH, liver transplantation is not considered to be a cure for AH, as it is accompanied by additional phases of care and health monitoring
Alcohol-Associated Clinical Trial Biomarkers
Before diving into the publication history and utility of K18 biomarkers in alcohol-related research, let’s first discuss four main areas of alcohol-associated clinical trials that require the use of early liver injury biomarkers:
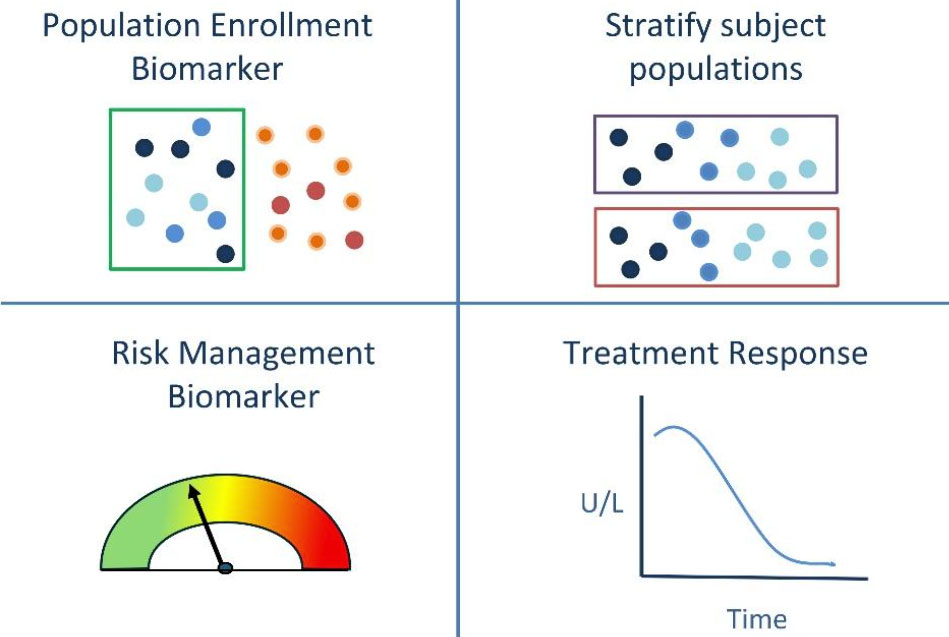
Population Enrollment Biomarkers
Exclude or include subjects with signs of early liver damage or significant liver damage such as AH. Population enrollment biomarkers could be utilized to identify subjects who have normal liver function laboratory tests (ALT, AST, etc.) yet show signs of significant liver injury via other diagnostics (elastography or biopsy).
Subject Stratification Biomarkers
Biomarkers are needed to generate balanced subject populations within treatment groups. These are also useful during comparative analysis studies to stratify subjects based on liver health biomarkers (ex. ALD vs. non-ALD) in order to determine the impact of different effects on various liver health backgrounds.
Risk Management Biomarkers
Risk management biomarkers measure the effectiveness of intervention studies to mitigate potential risks. ALD can progress silently, so early detection of liver injury can have meaningful impacts on liver health, enabling intervention before damage reaches advanced stages of liver disease. Intervention treatments and objectives can be tailored to subjects based on liver health risks. AUD intervention studies can leverage risk management biomarkers of liver health as motivators to prevent further liver damage and initiate steps toward preventing early-stage mortality that may arise from alcohol-driven liver disease.
Treatment Response
Liver injury biomarkers are needed to evaluate changes in liver health over the duration of treatment with the developmental drug. Treatment response biomarkers can be clinical indicators of treatment effectiveness regarding liver health outcomes in research studies. These could also include theragnostic biomarkers to predict response to treatment during clinical studies.
Cytokeratin-18: Liver Injury Biomarker
Cytokeratin-18 (CK18 or K18) is an intermediate filament protein in hepatocytes that is released into the circulation following liver injury and cell death (Ku et al. 2016). The measurement of K18 protein, detected by a combination of antibodies in the M65® ELISA kits (VLVbio, Sweden), can be used as an indicator of total cell death (Volkmann et al. 2008, Bantel et al. 2004). Induction of apoptosis drives increased levels of the caspase cleaved K18 fragment (ccK18) detected by the epitope specific M30® antibody (Bantel et al. 2004). Serum levels of ccK18 and K18 increase with liver injury severity (Chalin et al. 2023, Maccioni et al. 2023, McClain et al. 2021). A noteworthy publication record of clinical studies have investigated the capacities of ccK18 M30® and K18 M65® to function as liver injury biomarkers in alcohol-associated clinical studies. These clinical research studies have observed ccK18 M30® and K18 M65® in a variety of subject populations and target indications:
M65® & M30® for the Detection of early ALD, asymptomatic ASH, and AH
McClain et al. 2023, Vatsalya et al. 2023, Maccioni et al. 2023, Chalin et al. 2023,
McClain et al. 2021, Vatsalya et al. 2020, Atkinson et al. 2020, Bissonnette et al. 2017
M65® & M30® as Theragnostic Biomarkers for early ALD and AH
Sagaram et al. 2022, Atkinson et al. 2020
M65® as a Treatment Response Biomarker
McClain et al. 2023, Maccioni et al. 2023, Vatsalya et al. 2023
M65® & M30® as Prognostic Biomarkers of AH
Vatsalya et al. 2020, Atkinson et al. 2020, Woolbright et al. 2017
M65® & M30 correlate to Histological Stages of Disease Severity in ALD and AH
Maccioni et al. 2023, Atkinson et al. 2020, Mueller et al. 2017
Cytokeratin-18 in Alcohol-Associated Clinical Studies
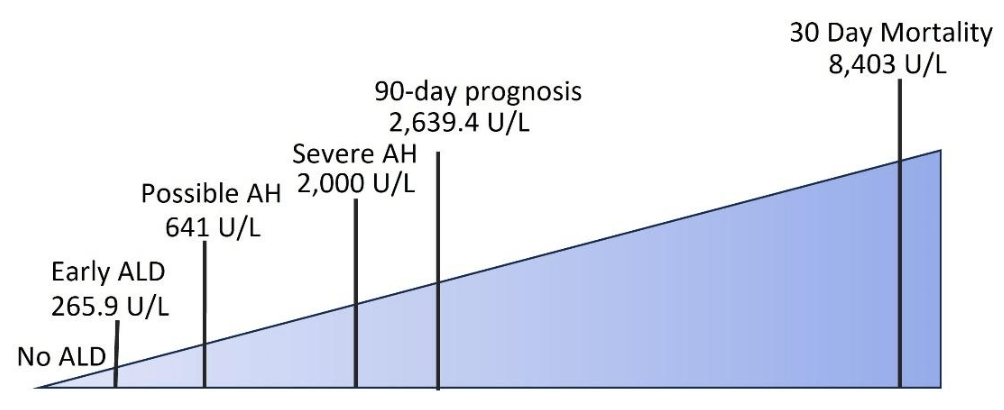
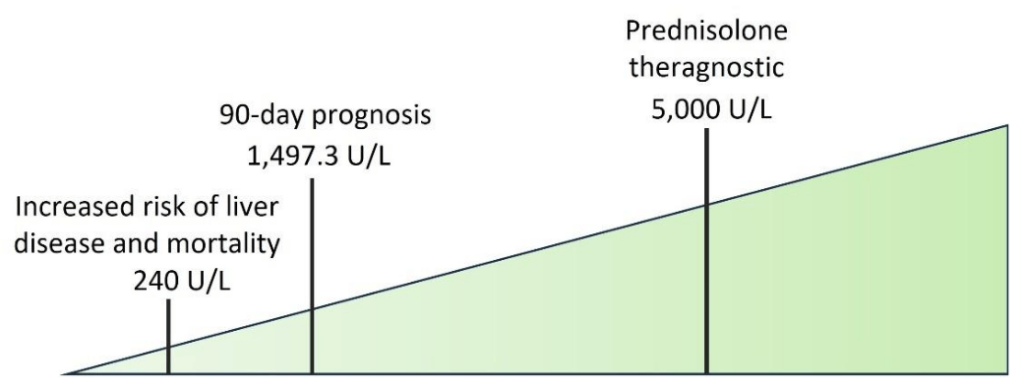
Published clinical research studies have carried these correlations further by suggesting cut-off values of ccK18 and K18 levels during the research investigation of alcohol-associated liver disease severity, theragnosis, and prognosis. (Fig. 1, Fig. 2, Table 1). It is important to consider that these suggested cut-offs were determined using two different kits that measure K18 levels, either the M65® ELISA K18 kit or the M65 EpiDeath® K18 kit from VLVbio (Nacka, Sweden) (Fig. 1). Of the two M65® kits, the M65 EpiDeath® K18 Kit has a broader range with higher sensitivity and specificity. This enables the M65 EpiDeath® K18 kit to more precisely discriminate between low, normal, and high K18 levels in these clinical research studies, as the kits are not for clinical use. Kit selection impacts data generation and how the data relates to other reported values. Additionally, various subject populations, enrollment criteria, and controls were used when determining these cut-off values. For the purposes of research in clinical trials, these proposed cut-off values lay an important foundation of findings to provide perspective when utilizing K18 biomarkers in alcohol-associated clinical trials (Table 1).
M65® in alcohol-associated liver disease research
M30® in alcohol-associated liver disease research
| Biomarker | Subject Population | Indication under Investigation | Suggested Cut-off Value | Study |
|---|---|---|---|---|
| M65® ELISA | AUD subjects admitted for elective alcohol withdrawal | Early ALD | 265.9 U/L | Maccioni et al. 2023 |
| M65 Epideath® | Subjects hospitalized for alcohol withdrawal | ASH | Lower: 323 U/L Upper: 2133 U/L | Chalin et al. 2023 |
| M65® ELISA | AUD subjects admitted for elective alcohol withdrawal | Progressive ALD (steatohepatitis or steatofibrosis) | 416 U/L | Macccioni et al. 2020 |
| M65® ELISA | Acute AH, AUD, and healthy controls | Clinically significant K18 levels | 500 U/L | Vatsalya et al. 2020 |
| M65 Epideath® | Subjects under clinical suspicion of AH | Possible AH | 641 U/L | Bissonette et al. 2017 |
| M65 Epideath® | Subjects under clinical suspicion of AH | Severe AH | 2,000 U/L | Bissonette et al. 2017 |
| M65® ELISA | Severe acute AH subjects | Favorable 90-day prognosis | ≤ 2629.4 U/L | Vatsalya et al. 2020 |
| M65 Epideath® | AH subjects | 30-day Mortality | 8,403 U/L | Woolbright et al. 2017 |
| M30 Apoptosense® | ALD subjects | Increased risk of liver disease and mortality | 240 U/L | Thorhauge et al. 2022 |
| M30 Apoptosense® | Severe acute AH subjects | Favorable 90-day prognosis | ≤ 1497.3 U/L | Vatsalya et al. 2020 |
| M30 Apoptosense® | Severe AH subjects | Prednisolone Theragnostic | 5,000 U/L | Atkinson et al. 2020 |
| M65® ELISA : ALT Ratio | Acute AH, AUD, and biopsy-determined NASH subjects | Distinguish AH from NASH | 25 | Vatsalya et al. 2020 |
FAQs about Cytokeratin-18 in Alcohol-Associated Clinical Studies
To dive deeper into the practical utility of K18 biomarkers in alcohol-associated clinical studies, we put together a list of common questions with answers derived from published clinical studies.
How are subject populations defined within alcohol-related clinical studies?
The NIAAA and the US Dietary Guidelines have published guidelines of recommended drinking levels, along with definitions of a standard drink, binge drinking, moderate drinking, and heavy drinking (CDC 2023, NIAAA 2024). These guidelines can be leveraged to define drinking populations within a study.
The diagnostic criteria defining the spectrum of AUD and ALDs, including alcohol-associated steatohepatitis (ASH) and AH, are available from AASLD and can be used to classify subject populations (Lucey et al. 2020).
Initial liver injury can be determined using traditional liver biomarkers, such as ALT levels. In one clinical study involving AUD subjects, initial ALT measurements were used to stratify study participants into two groups; those with liver injury and those without (Kirpich et al. 2017). However, it should be noted that limitations have been described in correlating ALT and AST levels to liver disease severity in certain liver disease populations (Vatsalya et al. 2020). Additional liver biomarkers, such as K18 which correlates with liver disease severity, could be considered for stratification of clinical study participants.
Liver morphology can define subject populations through liver histology (biopsy) or imaging techniques (Fibroscan). For instance, one clinical study characterized liver disease severity in AUD subjects using ALT levels and Fibroscan analysis (Maccioni et al. 2023). Minimal liver disease was defined as normal AST and ALT levels, normal liver stiffness, with or without the presence of steatosis (Maccioni et al. 2023). Early ALD populations were identified by elevated AST or ALT levels in addition to steatosis and/or increased liver stiffness (Maccioni et al. 2023). Thus, the combination of liver morphology analysis together with liver biomarker measurements could enhance population characterization within a clinical study.
Correlation analyses can interrogate the association of multiple variables within a study. These could include drinking consumption levels (number of drinks per drinking day), duration of drinking history (number of years of heavy drinking), alcohol biomarkers (PEth, blood alcohol content, etc.) and lifestyle factors as study variables for comparison (Kirpich et al. 2017, Thorhauge et al. 2022).
How quickly do K18 levels decrease following treatment?
The rate that K18 levels decrease following treatment likely depends upon several factors including the severity of liver injury, the effectiveness of treatment, and individual variability of subjects. Several studies measuring serum K18 levels via M65® ELISA analysis in alcohol dependent subjects during alcohol detoxification/abstinence showed a stepwise decrease in K18 over the span of 15 days (Kirpich et al. 2017), 2 weeks (Hartmann et al. 2021), and 3 weeks (Maccioni et al. 2020).
One group investigated this further in an early liver disease study of AUD subjects with ALD and fibrosis. Standard of care (SOC) treatment over the course of two weeks in this population indicated that individuals with ALD and fibrosis exhibited a statistically significant decrease in ccK18 levels detected via M30® from baseline following treatment in a clinical research study (Sagaram et al. 2022). Subjects who exhibited elevated baseline levels of K18, as detected with M65® ELISA, and who did not show improvement in K18 levels after 2 weeks SOC also had elevated FIB-4 at baseline (Sagaram et al. 2022). Elevated K18 levels at baseline indicate the presence of liver necrosis and should be considered with special attention when paired with the presence of fibrosis in early liver disease (Sagaram et al. 2022). This suggests that K18 and ccK18 levels could be used to differentiate AUD subjects with early ALD and baseline fibrosis who may not show improvement in liver injury following SOC treatment.
What sort of studies have been done to correlate K18 to liver histology?
Several research studies have shown a significant correlation of K18 M65® and ccK18 M30® biomarkers to liver histology. An early study investigating the potential for serum M30® and M65® levels to correlate to liver histology in a cohort of heavy drinkers showed that M65® correlated with ballooning, Mallory-Denk bodies, inflammation, steatosis, and fibrosis (Mueller et al. 2017). M30® correlated with histological signs of liver injury, ballooning, lobular inflammation, steatosis, and less so with fibrosis in this population of heavy drinkers (Mueller et al. 2017). ROC analysis indicated that M30® predicts hepatic steatosis (AUROC=0.843) while M65® predicts ballooning (AUROC=0.789) (Mueller et al. 2017).
In a population of subjects with AH, serum ccK18 M30® and K18 M65® levels correlated with histological severity of ASH and inflammation (Atkinson et al. 2020). Authors concluded that M30® and M65® reflect histological inflammation and injury with acute liver injury, while not showing strong correlations with liver fibrosis (Atkinson et al. 2020).
In further support of these findings, a recent study of a cohort of subjects with early ALD showed positive correlations of serum K18 M65® levels with the Study of Alcohol-related liVer disease in Europe (SALVE) histopathology activity grade, which encompasses hepatocellular and lobular inflammation, and no correlation with fibrosis (Maccioni et al. 2023). This agrees with the previous conclusions that K18 correlates with histological signs of liver injury, hepatocyte death, and inflammation, independent of fibrosis.
K18 levels correlate to liver histology. How quickly can histological changes, as indicated by K18 levels, be expected within a study?
Similar to changes following treatment, expected changes to histology as indicated by K18 levels depends on many factors. The severity of liver damage may impact how quickly the liver can regenerate. The efficacy and consistency of treatment will impact the improved histology of the liver. To our knowledge, no known studies have investigated the rate or speed of K18 biomarkers to reflect histological changes over time.
Do K18 values correlate with alcohol-associated liver disease severity?
A research study investigating alcohol-associated cirrhosis (AC) and AH suggested correlations between increased plasma ccK18 and K18 levels and disease severity in AC. Both ccK18 and K18, detected with M30® and M65® antibodies respectively, were further elevated in AH samples, with M65® being significantly higher than M30®. Mechanistically, this suggests that subjects with AC have significant levels of apoptotic cell death and subjects with AH have additional increases in necrotic cell death (Woolbright et al. 2017). Another study of subjects with suspected AH supported this finding. Plasma levels of ccK18 and K18 were significantly elevated in biopsy-confirmed AH compared to subjects without AH (Bissonette et al. 2017).
An additional large study analyzing AUD and AH samples found statistically significant positive correlations of increasing M30® and M65® levels with ALD severity (McClain et al. 2021). May it be noted that in this same study, AST and ALT levels showed limited utility in predicting liver disease severity within the moderate and severe AH populations (Vatsalya et al. 2020, McClain et al. 2021.)
Focusing on early indications of ALD, a clinical study analyzing K18 M65® measurements in AUD subjects determined that K18 M65® levels identified early forms of ALD compared to groups with minimal liver disease that had K18 M65® levels similar to healthy controls (Maccioni et al. 2023). Together, this research along with other clinical studies, support the correlation of K18 values to liver disease severity in AUD, ALD, and AH, although further research is needed to validate these findings.
Can K18 be used to distinguish types of liver injury or sources of liver injury, such as viral, chemical, metabolic, autoimmune, or alcohol-induced liver damage?
K18 is a powerful biomarker of liver injury and inflammation that does not specify between specific etiologies of liver disease. Thus, additional tests may need to be performed to distinguish between different types of liver injury and sources of liver injury. Viral serology tests can be used to identify the presence of viral infections. Toxicity testing can be performed to assess exposure to toxins or environmental chemicals. The presence of metabolic risk factors may suggest metabolic dysfunction-associated steatotic liver disease (MASLD) or metabolic dysfunction-associated steatohepatitis (MASH) as a source of liver injury and inflammation. Testing for the presence of autoantibodies can aid in the identification of autoimmune hepatitis. Reported alcohol consumption levels and alcohol biomarkers (PEth, etc.) may suggest alcohol as a driver of liver disease.
Metabolic alcohol-associated liver disease (MetALD) is a relatively new term created by the liver community to describe the synergistic impacts of metabolic risk factors combined with the influence of significant alcohol consumption. More studies need to be done to characterize K18 biomarker levels in metALD populations.
Further Reading
Peviva M30® Apoptosense® for ccK18 and Peviva M65® assays for total CK18 are labeled for Research Use Only (RUO) and are not intended for clinical diagnostic use. Any mention of clinical utility in this reference list is not supported by the manufacturer or distributor.
Atkinson, S. R., Grove, J. I., Liebig, S., Astbury, S., Vergis, N., Goldin, R., Quaglia, A., Bantel, H., Guha, I. N., Thursz, M. R., Newcombe, P., Strnad, P., & Aithal, G. P. (2020). In severe alcoholic hepatitis, serum keratin-18 fragments are diagnostic, prognostic, and theragnostic biomarkers. American Journal of Gastroenterology, 115(11), 1857–1868. https://doi.org/10.14309/ajg.0000000000000912
Bantel, H., Lügering, A., Heidemann, J., Volkmann, X., Poremba, C., Strassburg, C. P., Manns, M. P., & Schulze-Osthoff, K. (2004). Detection of apoptotic caspase activation in sera from patients with chronic HCV infection is associated with fibrotic liver injury. Hepatology, 40(5), 1078–1087. https://doi.org/10.1002/hep.20411
Bissonnette, J., Altamirano, J., Devue, C., Roux, O., Payancé, A., Lebrec, D., Bedossa, P., Valla, D., Durand, F., Ait‐Oufella, H., Sancho‐Bru, P., Caballeria, J., Ginès, P., Boulanger, C. M., Bataller, R., & Rautou, P. (2017). A prospective study of the utility of plasma biomarkers to diagnose alcoholic hepatitis. Hepatology, 66(2), 555–563. https://doi.org/10.1002/hep.29080
CDC: Alcohol questions and answers | cdc. (2023, March 23). https://www.cdc.gov/alcohol/faqs.htm
Chalin, A., Turlin, B., Ousmen, A., Michalak, S., Mueller, J., Mueller, S., Legros, L., Bardou‐Jacquet, E., Viel, J. F., Samson, M., & Moirand, R. (2023). Non‐invasive diagnosis of alcohol‐related steatohepatitis in patients ongoing alcohol withdrawal based on cytokeratin 18 and transient elastography. Alimentary Pharmacology & Therapeutics, 58(1), 80–88. https://doi.org/10.1111/apt.17515
Hartmann, P., Lang, S., Zeng, S., Duan, Y., Zhang, X., Wang, Y., Bondareva, M., Kruglov, A., Fouts, D. E., Stärkel, P., & Schnabl, B. (2021). Dynamic changes of the fungal microbiome in alcohol use disorder. Frontiers in Physiology, 12, 699253. https://doi.org/10.3389/fphys.2021.699253
Kirpich, I. A., McClain, C. J., Vatsalya, V., Schwandt, M., Phillips, M., Falkner, K. C., Zhang, L., Harwell, C., George, D. T., & Umhau, J. C. (2017). Liver injury and endotoxemia in male and female alcohol‐dependent individuals admitted to an alcohol treatment program. Alcoholism: Clinical and Experimental Research, 41(4), 747–757. https://doi.org/10.1111/acer.13346
Ku, N., Strnad, P., Bantel, H., & Omary, M. B. (2016). Keratins: Biomarkers and modulators of apoptotic and necrotic cell death in the liver. Hepatology, 64(3), 966–976. https://doi.org/10.1002/hep.28493
Lucey, M. R., Im, G. Y., Mellinger, J. L., Szabo, G., & Crabb, D. W. (2020). Introducing the 2019 american association for the study of liver diseases guidance on alcohol‐associated liver disease. Liver Transplantation, 26(1), 14–16. https://doi.org/10.1002/lt.25600
Maccioni, L., Horsmans, Y., Leclercq, I., Schnabl, B., & Stärkel, P. (2023). Serum keratin 18‐M65 levels detect progressive forms of alcohol‐associated liver disease in early noncirrhotic stages. Alcohol: Clinical and Experimental Research, 47(6), 1079–1087. https://doi.org/10.1111/acer.15081
McClain, C. J., Kirpich, I., Song, M., & Vatsalya, V. (2023). Keratin 18‐M65: A biomarker for early‐stage alcohol‐associated liver disease. Alcohol: Clinical and Experimental Research, 47(7), 1257–1260. https://doi.org/10.1111/acer.15117
McClain, C. J., Vatsalya, V., & Mitchell, M. C. (2021). Keratin-18: Diagnostic, prognostic, and theragnostic for alcohol-associated hepatitis. American Journal of Gastroenterology, 116(1), 77–79. https://doi.org/10.14309/ajg.0000000000001042
Mueller, S., Nahon, P., Rausch, V., Peccerella, T., Silva, I., Yagmur, E., Straub, B. K., Lackner, C., Seitz, H. K., Rufat, P., Sutton, A., Bantel, H., & Longerich, T. (2017). Caspase‐cleaved keratin‐18 fragments increase during alcohol withdrawal and predict liver‐related death in patients with alcoholic liver disease. Hepatology, 66(1), 96–107. https://doi.org/10.1002/hep.29099
NIAAA: The basics: Defining how much alcohol is too much | national institute on alcohol abuse and alcoholism(NIAAA). (n.d.). Retrieved February 6, 2024, from https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/basics-defining-how-much-alcohol-too-much
Sagaram, M., Parthasarathy, R., Condon, S. L., Closson, C. F., Kong, M., Schwandt, M. L., Jophlin, L. L., Feng, W., Barve, A. J., & Vatsalya, V. (2022). Theragnostic efficacy of k18 response in alcohol use disorder with clinically significant fibrosis using gut-liver axis. International Journal of Molecular Sciences, 23(10), 5852. https://doi.org/10.3390/ijms23105852
Thorhauge, K. H., Thiele, M., Detlefsen, S., Rasmussen, D. N., Johansen, S., Madsen, B. S., Antonsen, S., Rasmussen, L. M., Lindvig, K. P., & Krag, A. (2022). Serum keratin‐18 detects hepatic inflammation and predicts progression in compensated alcohol‐associated liver disease. Hepatology Communications, 6(12), 3421–3432. https://doi.org/10.1002/hep4.2075
Vatsalya, V., Cave, M. C., Kong, M., Gobejishvili, L., Falkner, K. C., Craycroft, J., Mitchell, M., Szabo, G., McCullough, A., Dasarathy, S., Radaeva, S., Barton, B., & McClain, C. J. (2020). Keratin 18 is a diagnostic and prognostic factor for acute alcoholic hepatitis. Clinical Gastroenterology and Hepatology, 18(9), 2046–2054. https://doi.org/10.1016/j.cgh.2019.11.050
Vatsalya, V., Royer, A. J., Jha, S. K., Parthasarathy, R., Tiwari, H., Feng, W., Ramchandani, V. A., Kirpich, I. A., & McClain, C. J. (2023). Drinking and laboratory biomarkers, and nutritional status characterize the clinical presentation of early-stage alcohol-associated liver disease. In Advances in Clinical Chemistry (Vol. 114, pp. 83–108). Elsevier. https://doi.org/10.1016/bs.acc.2023.02.001
Volkmann, X., Anstaett, M., Hadem, J., Stiefel, P., Bahr, M. J., Lehner, F., Manns, M. P., Schulze-Osthoff, K., & Bantel, H. (2008). Caspase activation is associated with spontaneous recovery from acute liver failure. Hepatology, 47(5), 1624–1633. https://doi.org/10.1002/hep.22237
Winrich, E. J., Gala, K. S., Rajhans, A., Rios-Perez, C. D., Royer, A. J., Zamani, Z., Parthasarathy, R., Marsano-Obando, L. S., Barve, A. J., Schwandt, M. L., & Vatsalya, V. (2022). Association of hypomagnesemia and liver injury, role of gut-barrier dysfunction and inflammation: Efficacy of abstinence, and 2-week medical management in alcohol use disorder patients. International Journal of Molecular Sciences, 23(19), 11332. https://doi.org/10.3390/ijms231911332
Woolbright, B. L., Bridges, B. W., Dunn, W., Olson, J. C., Weinman, S. A., & Jaeschke, H. (2017). Cell death and prognosis of mortality in alcoholic hepatitis patients using plasma keratin-18. Gene Expression, 17(4), 301–312. https://doi.org/10.3727/105221617X15016197658871