The Chromogenic Factor X Assay (CFX)
Posted on: December 10, 2019
David L. McGlasson, MS, MLS(ASCP)
Posted: December 10, 2019
This month’s Clot Club entry discusses the chromogenic Factor X assay. What is it? And how is it different from the anti-FXa assay?
MONITORING WARFARIN THERAPY, DIRECT THROMBIN INHIBITORS (DTI), AND SUBJECTS ON ORAL ANTICOAGULANT THERAPY (OAT) WITH INTERFERING SUBSTANCES SUCH AS MEDICATIONS AND NON-SPECIFIC INHIBITORS SUCH AS LUPUS ANTICOAGULANTS (LA).
Quite a long title wasn’t it. I’m going to take you back a bit in years and go through the evolution of using the chromogenic Factor X (CFX) method for monitoring subjects on anticoagulants where clottable assays may not be adequate to maintain the proper therapy for individual patients.
In 1997 Stephan Moll MD and Thomas L. Ortel MD, PhD., wrote one of the first papers to question the adequacy of the of the therapeutic International normalized ratio (INR) for oral anticoagulants in subjects who had the presence of an LA and had a thromboembolic event. Patients who have a Lupus Anticoagulant (LA) often have a prolonged prothrombin time (PT) and an elevated INR. They looked at alternate methods to use in monitoring warfarin therapy in this subgroup of patients. They looked at 34 subjects who had the presence of a LA. They then used several methods to measure the effects of the LA on different methods on subjects who were on warfarin and another group who had the inhibitor but were not receiving warfarin.
They used a PT using different manufacturer’s thromboplastin with INR’s calculated with each reagent/instrument combination on the subjects receiving warfarin. They also assayed coagulation FII, CFX, and prothrombin-proconvertin (P-P) times that were performed on subjects receiving warfarin.
On subjects with the presence of an LA not getting warfarin the PTs were often prolonged and had a great variation in times depending on the different manufacturer’s thromboplastin reagent. Different thromboplastins which differed in sensitivity to the presence of an LA and were receiving warfarin the INRs greatly varied in values. These results also overestimated the extent of anticoagulation. The CFX levels and the P-P times correlated well with their results and with therapeutic ranges that had already been established.
Their conclusions were that presence of an LA can interfere with different assays and cause inaccurate INRs that do not reflect the accuracy of anticoagulation. They recommended that to prevent subtherapeutic or supratherapeutic anticoagulation a method must be used that is insensitive to the presence of an LA. Since the P-P test is no longer used in many laboratories the CFX is the recommended method of choice.1
The different values of PT/INR results in different reagent/instrument combinations was later seen in a protocol conducted in our facility that tested 12 different reagent/instrument combinations on normal subjects, patients with an LA presence, unfractionated heparin therapy and on warfarin therapy. All of the reagent/instrument combinations had a local calibration of thromboplastin international sensitivity indexes (ISI) performed before testing.
The differences between manufacturer versus local calibrated ISI ranged from 0.9-18.9% for normal sample INRs and from 0.8-16.4% on patient samples INRs. The number (or proportion) of patient specimens with clinically significantly different INR values (>10.0% difference) ranged from zero for several reagent combinations to more than half (or >50.0%) of those tested for several other combinations. These results also make a case that if you are using a clottable assay such as the PT/INR local calibration should be accomplished when comparing results from different facilities before comparing INR values in subjects on OAT2
In 2000 Mike Sanfelippo commented on a series of patients with the presence on an LA in who the PT was affected by the LA. This caused an artifactually increased INR. The subjects were identified by failure to correct mixing studies with normal plasma and the subject’s plasma with a 1:1 mix and a CFX level discordant with the PT/INR. His group suggested that patients on OAT with this issue be monitored with the CFX method to control their anticoagulation instead of the PT/INR. Patients who have this complication may result in inadequate anticoagulation and have recurrent thrombotic issues.3
Jumping forward to 2004 Rosborough and Shepherd performed a study to compare the INRs of patients positive for LA and the INRs of control subjects receiving OAT with simultaneous therapeutic CFX levels. They used 68 patients who were positive for the presence of an LA and 57 control subjects who were receiving long-term OAT therapy.
They measured INR values and CFX activity on all subjects. They found in 44 control patients (77%) and 46 patients with LAs present (68%), CFX activity was 22-40% of normal which is therapeutic. Of the 44 control patients 4 (9%) had an INR above 3.0 and now had an INR above 4.0. In contrast, 18(39%) of the 46 patients with LAs had an INR above 3.0, and 5(11%) had an INR above 4.0.
Of the subjects with LAs receiving OAT 10% may have falsely high INR values, which may lead to inaccurate OAT dosing reduction. The use of the CFX method in monitoring subjects on OAT with the presence of an LA avoids this INR interfering substance.4
In 2005 Arpino performed a protocol to determine the use of the CFX assay to predict the INR in subjects that were transitioning from argatroban, a direct thrombin inhibitor (DTI), to warfarin. The study purpose was to determine if the CFX levels were suitable when converting the subjects from the DTI to the OAT Vitamin K agonist.
Sixty-two in-patients who were anticoagulated with argatroban were used in this study who were to be converted to warfarin and were monitored with the CFX method. For 6 months the data for all patients who were monitored with the CFX was used to convert from argatroban to warfarin. When the CFX levels were in satisfactory range the clinician discontinued the argatroban and a confirmatory INR was obtained.
They determined the ability of the CFX results to predict the INR free of the DTI influence. They calculated the CFX level of 45% or less to correspond to an INR of 2 or less and the CFX less than 45% as greater than the INR of 2.0. They used a receiver-operator-curve (ROC) to illustrate various cutoff levels of CFX. Of 146 patients screened, 62 had data that met criteria for analysis. They found an average of 6+/-3 doses of warfarin were administered and the CFX/INR studies were obtained. The average time of measurement was 9+/-4 hours. The sensitivity of the CFX level of 45% or less to predict an INR. A CFX level of 45% or less to predict and INR of 2 or greater absent of argatroban influence had a sensitivity of 93%, a specificity of 78%, and an accuracy of 89%. The area under the ROC was 0.91. They concluded the CFX level was an accurate method alternative with a level of 45% or less is a reliable predictor that the INR will then be therapeutic after discontinuing argatroban.5
In 2008 DL McGlasson performed a study for comparison of a CFX assay with INR for monitoring oral anticoagulation therapy. The purpose of the present study was to compare the international normalized ratio with a chromogenic factor X (CFX) assay for monitoring patients on oral anticoagulant therapy using the DiaPharma CFX method on a STA-R Evolution coagulation analyzer.
International normalized ratio values were correlated with the CFX for determining normal, subtherapeutic, therapeutic and supratherapeutic ranges for these patients. Specimens were analyzed and grouped as normal or patients on oral anticoagulant therapy with international normalized ratios of less than 2.0, 2.0-3.0, and more than 3.0.
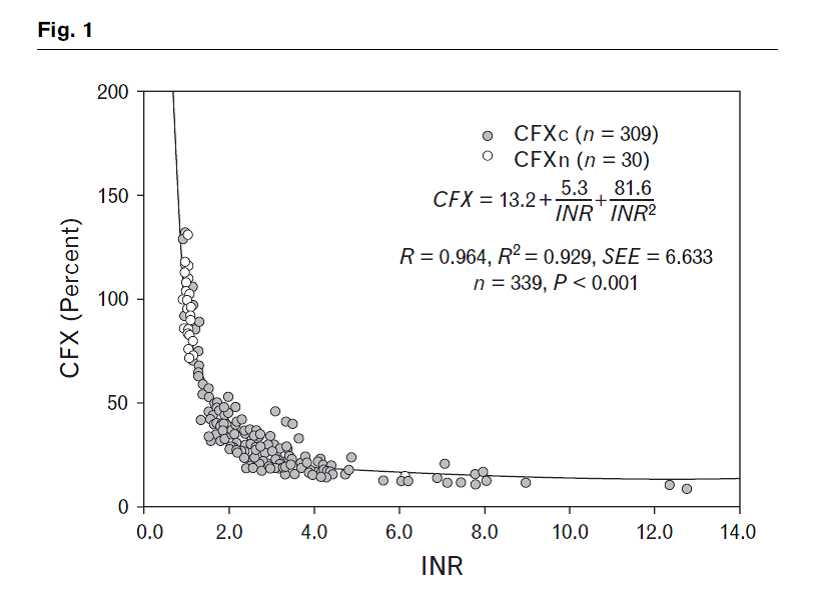
Three hundred and nine randomly selected oral anticoagulant therapy patients were tested. The range of INR and CFX in oral anticoagulant therapy patients was 0.92-12.76 and 9-132%, respectively. CFX was inversely related to international normalized ratio; R = 0.964 (P < 0.0001) (CFX = 13.2 + (5.3/international normalized ratio) + (81.3/international normalized ratio).
Results by group were as follows: normal (n = 30), CFX range 72-131%, mean CFX 96%; international normalized ratio less than 2.0 (n = 70), CFX range 32-132%, mean CFX 53%; international normalized ratio 2.0-3.0 (n = 135), CFX range 18-48%, mean CFX 28%; international normalized ratio more than 3.0 (n = 104), CFX range 9-46%, mean CFX 21%. Sensitivity and specificity crossed at a CFX of 35.5%, which yielded a sensitivity of 91.7% and a specificity of 91.9% for discriminating international normalized ratio of at least 2.0. Area under the curve on receiver-operator curve using international normalized ratio was 0.984 (P < 0.001).
In this randomly selected group of oral anticoagulant therapy patients and normal individuals at varying levels of anticoagulation, CFX correlated well with international normalized ratio as determined by R = 0.964. The data suggests that the CFX can be a useful tool for monitoring oral anticoagulation in patient populations in which confounders to international normalized ratio may be present. Further investigation with the use of CFX for monitoring is warranted in large patient populations on oral anticoagulant therapy, including follow-up for clinical outcomes.6
See the Figure below which indicates that small changes in factor X above INR 4.5 produce large changes in INR.
This data shows that the “flattening out” of the curve of the INR renders the results suspect in the “Supratherapeutic range” (above 4.5). This makes the CFX to be considered as the alternative to the INR when measuring the levels of OAT treatment dosing.
Moving along in 2009 M Sanfelippo discussed the use of CFX to accept or reject INR results in warfarin treated patients. A warfarin treated patient unexpectedly presented with an elevated INR. Repeat testing in two laboratories gave conflicting results. The chromogenic assay of factor X was used to determine the correct INR result. The patient had laboratory results consistent with a dysfibrinogenemia, which prevented detection of the endpoint with a photo-optical detection system. The CFX assay of factor X is recommended for monitoring patients on warfarin when the INR cannot be accurately determined due to interference with the fibrin endpoint in the INR.7
In 2009 TK Rosborough also researched the relationship between CFX and INR differences during early warfarin initiation compared with chromic warfarin administration. CFX monitoring is necessary in patients with potential INR artifacts during warfarin therapy. The relationship of CFX with the INR needs to be quantitated to have warfarin protocols that are equivalent with either test as a monitoring parameter. This study investigated whether the CFX/INR relationship is different during warfarin initiation compared with that during chronic warfarin therapy. Outpatients (N = 164) taking chronic doses of warfarin and inpatients (N = 137) initiating warfarin therapy had plasma samples tested for CFX and INR. The best fit mathematical relationship of CFX and INR was determined for both groups. A six hundred and twenty-five bed, adult-only, private, tertiary care teaching hospital was the setting of the study. The best fit equation for chronic warfarin patients was quadratic using a reciprocal transformation of the INR. The best fit equation for the warfarin initiation patients was linear using logarithmic transformation of CFX and INR. The predicted CFX from INRs over the range of 1.4-2.2 was 7-18% higher in the warfarin initiation patients than in the chronic warfarin patients. Translation of CFX values into equivalent INRs for use in warfarin initiation and maintenance protocols is improved when using equations specific to the patient situation. Rosborough’s group also saw the same issues discovered by McGlasson et al in the elevated INR’s not being truly predictable as to the patients true therapeutic INR results in comparison to the CFX levels.8
In 2010 Rosborough again revisited the use of the CFX in warfarin treated patients. They looked at FX and FII activity levels do not always agree in warfarin-treated LA patients. Warfarin therapy is used in lupus anticoagulant patients with thrombosis and yet the prothrombin time (PT)/international normalized ratio (INR) in these patients can sometimes be falsely elevated. Both a PT-based factor II (FII) assay and a chromogenic, enzymatic factor X (CFX) assay have been used for monitoring when the INR may be artifactual.
This study compared FII and CFX assays in LA-positive and LA-negative warfarin-treated patients in a cross-sectional study of samples from 21 LA and 19 LA-negative outpatients. Plasma samples were simultaneously measured for FII and CFX and the ratio of FII/CFX was used to measure concordance. Compared with LA-negative patients 14 of the 21 LA-positive patients had lower FII/CFX ratios (P < 0.01). Three of the patients had ratios less than 0.6 indicating strong disagreement (P < 0.0001). The patient with the lowest FII/CFX ratio had evidence suggesting a specific antibody to FII. Another patient showed that the discordance between FII and CFX varied over time. The CFX assay in the laboratory was technically superior, more precise, and less costly.
Again, this protocol has found the CFX assay is preferred for warfarin therapy monitoring in LA patients when INR interfering substances are suspected.8
In 2010 M Balaban et al: first proposed the use of the CFX to monitor the “New Oral Anticoagulants” which are now known as the direct oral anticoagulants (DOACs) in subjects with the presence of antiphospholipid antibody syndrome (APA).
Their purpose was to determine the validity of the (INR) and prothrombin time (PT) as a monitor for warfarin therapy in patients with LAs and recurrent thrombosis, and to investigate alternative approaches to monitoring warfarin therapy and new treatment options in these patients.
A case is described of a 63-year-old female with antiphospholipid syndrome and recurrent venous thrombosis despite optimal adjusted warfarin therapy. In patients with LAs, the INRs obtained while receiving warfarin vary and often overestimate the extent of anticoagulation, while PT without receiving warfarin is often prolonged.
In conclusion, LAs can influence PT and lead to INR that does not accurately reflect the true level of anticoagulation. Optimizing of (warfarin) OAT could be achieved by individual monitoring of anticoagulation effect with a test that is insensitive to LAs (CFX assay). Emerging oral anticoagulants, direct thrombin inhibitors and direct factor Xa inhibitors, such as dabigatran and rivaroxaban, with a predictable anticoagulant response and little potential for food or drug interactions, have been designed to be administered in fixed doses without coagulation monitoring and could be the treatment choice for these patients.9
The previous material has now brought us up to issues with measuring the DOACs on subjects with LAs and suggesting these medications could be helpful in treating these subjects. Again, the CFX assay is brought up and for the first time suggests that this assay could be used to help monitor these patients. So we now have tests out there with acronyms relating to coagulation FX. Wool and Lu in 2013 have suggested the pathology consultation on anticoagulation monitoring should be done when using factor-X related assays to ease the confusion when ordering and interpretation of these tests.
Their purpose was to review various anticoagulation therapies and related laboratory monitoring issues, with a focus on factor X-related chromogenic assays.
They used a case-based approach to review pertinent published literatures and product inserts of anticoagulation drugs and to look back on clinical use of factor X-related chromogenic assays.
The number of anticoagulants available to clinicians has increased greatly in the past decade. Whether and how these anticoagulants should be monitored are areas of uncertainty for clinicians, which can lead to misuse of laboratory assays and suboptimal patient management. Factor X-related assays are of particular concern because of the similar and often confusing test names. Based on a common clinical case scenario and literature review regarding anticoagulant monitoring, an up-to-date discussion and review of the various factor X-related assays are provided, focusing on the differences in test designs and clinical utilities between the chromogenic anti-Xa and CF X activity assays.
They concluded anticoagulation therapy and related laboratory monitoring are rapidly evolving areas of clinical practices. A good knowledge of relevant laboratory assays and their clinical applications is necessary to help optimize patient care.10
I personally was involved in problems with physicians and nurses in ordering anti-FXa testing in heparin monitoring. Many times we would get an order for a FX assay when they really wanted an anti-FXa method to monitor a patient on some heparinoid. It actually led to me being involved in developing the single calibration or ”hybrid curve” for monitoring numerous heparinoids years ago after frustration in these matters.
See: McGlasson DL. Monitoring Unfractionated Heparin and Low Molecular Weight Heparin Anticoagulation with an anti-Xa Chromogenic Assay using a Single Calibration Curve. Lab Medicine. 2005;36(5):297-299.
McGlasson DL et al: Effects of Pre-analytical Variables on the anti-Fxa Chromogenic Assay when Monitoring Unfractionated Heparin and Molecular Weight Heparin Anticoagulation. Blood Coagulation and Fibrinolysis. 2005;16(3):173-176
In 2014 Crowl and associates published a review article on warfarin monitoring in APS and LAs. Their purpose was to review the literature that was present on INR and CF monitoring in subjects with APS specifically LA and to identify the benefits of one monitoring method compared with the other in the presence of an LA.
A literature search was conducted through MEDLINE (1946-May 2014) utilizing the following MeSH terms chromogenic compounds, anticoagulants, and factor X. Further articles were identified from original literature citations.
All English-language studies were included that involved INR and/or CFX monitoring in APS patients that focused on a therapeutic anticoagulation level with warfarin therapy.
A total of 55 articles were identified, of which nine are referenced because of their relevance for this review: three articles focus on the efficacy of utilizing INR monitoring in patients with APS, five focus on CFX compared with INR for therapeutic warfarin dosing, and one compares different thromboplastins utilizing both INR and CFX monitoring. INR monitoring in patients with APS, specifically LA, was not found to be reliable because thromboplastin reagents are sensitive to LA. Furthermore, when INR was compared to CFX, patients with LA had supratherapeutic INRs despite having CFX within goal range.
The investigators concluded that in a subgroup of APS patients, INR monitoring may not be safe for determining the dose of warfarin because their INR values can be falsely elevated. Preferably the CFX levels between 20-40% is the desired therapeutic range when the INR is inaccurate. Although CFX monitoring is more accurate, it too comes with its own downsides. Managing warfarin therapy in the APS population needs to be individualized.11
A Dush and H Paige now bring us up to date in 2019 with questions in monitoring point-of-care testing (POC) in patients with the presence of APS/LA.
Management of patients with APS on warfarin therapy can be extremely difficult. The INR of patients with APS can be falsely elevated. This elevation is thought to be reflective of the reaction of the antiphospholipid antibody with the thromboplastin used to measure the PT. We have discussed this issue previously. This false elevation can be seen in both venipuncture testing (VP) and POC results. This discrepancy is usually more apparent in patients with whose INR is tested using a POC device. As a result, there is a preference for VP/INR testing in most patients with APS requiring warfarin therapy. In this case they discuss one patient who they correlated the VP-INR with POC-INR as well as a chromogenic factor X level in order to manage the subjects INR by POC-INR testing.
Correlation testing was performed at 3 time points: baseline, 2 months and 6 months.
| Correlation Points | VP-INR | POCT-INR | CFX%) |
| 1-baseline | 2.1 | 2.5 | 34 |
| 2-2 months | 2.4 | 3.0 | |
| 3-6 months | 2.8 | 4.1 |
The investigators used a derived change of the POC INR unique to this patient with a goal of an INR range of 2.5-3.0 to account for the INR elevation.
The investigators stated “in carefully stated patients, correlating the VP and POC INR along with the CFX levels may allow these patients to be managed by POC INR.” However, this system would need to be performed for each individual patient correlation.12
In summary in the literature and laboratory practice the CFX is a robust assay that can assist physicians in treating subjects with APS/LA inhibitors and DTI conversion to OAT treatments. This assay can be set-up on many automated coagulation analyzers as well as being performed as a microtiter plate.
Performing the Chromogenic Factor X Assay (CFX)
PRINCIPLE: Coagulation Factor X is a Vitamin-K dependent protein produced by the liver. It has a central position in the coagulation cascade. Factor X is activated both by the extrinsic and intrinsic systems before exerting its effect on the conversion of prothrombin to thrombin. Patients who need anticoagulation therapy can be treated with warfarin, which is a vitamin K antagonist. This treatment leads to a decrease in all vitamin K dependent clotting factors and thus a prolonged clotting time of blood. The therapy requires careful monitoring since it is essential to find an optimal balance between risk of thrombosis and risk of careful monitoring since it is essential to find an optimal balance between risk of thrombosis and risk of bleeding for each patient. This assay may be a useful tool in the management of patients with lupus inhibitors receiving warfarin therapy and individuals with interfering substances. It also may be used when the conventional prothrombin time/INR testing may not be suitable for individual patients. The CFX assay is also a valuable tool when subjects are transitioned from a direct thrombin inhibitor to warfarin.
Measurement principle:
| RVV | ||
| FX | ———> | FXa |
| CaCl2 |
| FXa | ||
| S-2765 chromogenic | ———> | Peptide+pNA |
Reagents:
Sealed reagents are stable at 2-8⁰C until the manufacturer’s expiration date on the label. S-2765 25mg lyophilized chromogenic FXa substrate with mannitol added as a bulking agent. Reconstitute with 20 ml of sterile water. The reconstituted substrate is stable for 6 months when stored at 2-8⁰C.
Russell’s Viper Venom (RVV) 1.0 mg lyophilized FX activating protein from RVV. Reconstitute with 15 mL of sterile water. The reconstituted substrate is stable for 6 months when stored at 2-8⁰C.
CaCl2 . 0.1mol/L Calcium chloride solution. The prepared solution is stable at 2-4-⁰C until the manufacturer-s expiration date on the label.
Buffer. 100 mL buffer solution containing 0.05 mol/L Tris, pH 7.8 and 20.0 mg/L polybrene (hexadimethrine bromide). Ready for use. The buffer is stable at 2-8⁰C until the manufacturer’s expiration date on the label.
RVV+CaCl2. Before use mix 1 volume of RVV with 1 volume of CaCl2. The mixture is stable for 48 hours at 2-8C.
Commercial normal and abnormal quality controls and calibrators assayed against an international standard for CFX should be used. Every laboratory should establish their own ranges. Controls should be performed every 8 hours per shift according to good laboratory practices. Refer to Westgaard et al for dealing with out of control issues. The stability or the calibration should also be determined by each laboratory.
In my lab, I used STA-Unicalibrator (Stago, #00675): Freeze-dried citrated human plasma. This plasma is intended for use as a calibration plasma for functional assays. Reconstitute each vial with 1.0 mL reagent grade water and allow to equilibrate for 30 minutes at room temperature. Swirl gently. Stability on the STA-R Evolution is 4 hours.
STA-System Control N+P (Stago, #00678): Control N is citrated normal human plasma and Control P is citrated abnormal human plasma, both freeze-dried. Reconstitute each vial with 1.0 ml of reagent grade water and allow to equilibrate for 30 minutes at room temperature. Swirl gently. Stability on the STA-R Evolution is 4 hours.
SPECIMEN
Citrated Blood 9:1 (blood to anticoagulant) 3.2 % sodium citrate.
Follow CLSI guidelines H21-A5, 28(5), Fifth Edition. No other anticoagulant is
acceptable.
| Centrifugation: |
15 minutes at 2,500g; perform double centrifugation. Plasma should be platelet-poor (less than 10,000/cm3). |
||
| Plasma Storage: |
4 hours at 20 C 2 weeks at –20 C 6 months at –70 C Frozen plasma should be rapidly thawed only once at 37 C for 5 minutes and tested immediately. |
||
Unacceptable specimens: Samples that are short draws, clotted or hemolyzed may yield incorrect results.
Administration of Vitamin -K dependent or direct oral anticoagulants anti-IIa or anti-FXa inhibitors, heparinoids or direct thrombin inhibitors can influence any coagulation assay. Information on the time of the dosing of any anticoagulant medication should accompany the specimen.
CALIBRATION
A standard curve is required for each DiaPharma chromogenic FX test. Six standards must be included in each test run. For standardization use assigned calibrator plasma.
For example, in my lab, I used FX unicalibrator value of 157.0% activity obtained from Stago. (Future values may be slightly greater or less than 157.0%.)
Standard calibration curves preparation can be accomplished in the following manner after an initial equipment procedure test-set-up on the STA-R Evolution. The instrument will then serially dilute the unicalibrator in the following manner starting with a 1:7 dilution:
| FX% | DILUTION |
| 157 | 1/7 |
| 110 | 1/10 |
| 55 | 1/20 |
| 28 | 1/40 |
| 14 | 1/80 |
| 7 | 1/160 |
QUALITY CONTROL
Run a Quality Control such as System N&P normal and abnormal control with each run of specimens. All controls must be in the established ranges.
Each reagent/instrument should have an established and validated procedure in place before results can be reported. A full procedure for this method with various instrumentation be obtained on request.
CALCULATIONS
All test results are calculated automatically according to the procedure being performed.
Factor assays and chromogenic test results are calculated from standard curves. These curves are in the SYSTEM PANEL screen. Refer to icon for that and go to curve icon for results.
REPORTING RESULTS:
Chromogenic factor assays are reported out in percent (%) activity or international units (IU/L).
PROCEDURE NOTES:
In order for the test results to be considered valid, all of the criteria listed below must be met. If any of these are not met, the test should be considered invalid and the assay repeated.
The absorbance of the FX:Chr Calibrator 100.0% activity must be greater than 0.500.
The correlation coefficient of the standard curve must be greater than 0.9800.
The FX:Chr control concentration must be within the stated range.
LIMITATIONS OF THE PROCEDURE:
The assay has been used in a large number of patient studies without any reported drug interference. Heparin concentrations above 30U/mL are not neutralized by the polybrene and may influence the assay. Extremely elevated levels of bilirubin and plasma from hyperlipemic patients may give difficulties in absorbance readings. Dilutions of the plasma will have to be accomplished if this situation exists and results adjusted accordingly.
REFERENCES:
- Moll S, Ortel TL. Monitoring warfarin therapy in patients with lupus anticoagulants. Ann Intern Med 1997;127:177-185.
- McGlasson DL. A comparison of INRs after local calibration of thromboplastin international sensitivity indexes. Clin Lab Sci 2002;15(2):91-5.
- Sanfelippo MJ, Sennet J, McMahon EJ. Falsely elevated INRs in warfarin-treated patients with the lupus anticoagulant. WMJ 2000;99(3):62-4, 43.
- Rosborough TK, Shepherd MF. Pharmacotherapy 2004; Unreliability of International Normalized Ratio for Monitoring Warfarin Therapy in Patients with Lupus anticoagulant. Pharmacotherapy 2004;24(7):838-842.
- Arpino PA, Demirijan Z, Van Cott EM. Use of the chromogenic factor X assay to predict the Intenational normalized ratio in patients transitioning from argatroban to warfarin. Pharmacotherapy 2005;25(2):157-64.
- McGlasson DL, Romick BG, Rubal BJ. Comparison of a chromogenic factor X assay with international normalized ratio for monitoring oral anticoagulation therapy. Blood Coagulation and Fibrinolysis 2008, 19:513-517.
- Sanfelippo MJ, Zinsmaster W, Scherr DL, Shaw GR. Use of chromogenic Assay of Factor X to Accept or Reject INR Results in Warfarin Treated Patients. Clin Med and Research 2009;7:103-105.
- Rosborough TK, Jacobsen JM, Shepherd MF. Relationship between chromogenic factor X and international ratio differs during early warfarin initiation compared with chronic warfarin administration. Blood Coagulation and Fibrinolysis 2009;20:433-435
- Rosborough TK, Jacobsen JM, Shepherd MF. Factor X and factor II activity levels do not always agree in warfarin-treated lupus anticoagulant patients. Blood Coagul Fibrinolysis. 2010;21(3):242-4.
- Balaban M. et al: Recurrent venous thrombosis despite ‘optimal anticoagulation therapy’ for antiphospholipid syndrome-could new oral anticoagulants solve the problem? Acta Clin Croat. 2010;49(4):469-77.
- Wool GD, Lu CM Pathology consultation on anticoagulation monitoring: Factor X-related assays. Am J Clin Pathol 2013;140(5):623-34.
- Crowl A, Schullo-Feuiner A, Moon JY. Warfarin monitoring in antiphospholipid syndrome and lupus anticoagulant. Ann Pharmacother. 2014;48(11):1479-83.
- Dush A, Erdedeljac HP. INR Management of an Antiphospholipid Syndrome Patient With Point-of-Care INR Testing. J Pharm Pract 2019 Mar 27;897
ML-00-00533Rev01